
A 60 yo male is brought into the Emergency Department following collapsing at work.
On arrival he is alert and oriented with a heart rate of 20bpm, BP of 105/70 and a respiratory rate of 16.
He has no chest pain or other concerning features.
His past history includes:
- Atrial Fibrillation (on Sotalol and a NOAC)
- Hypercholesterolaemia
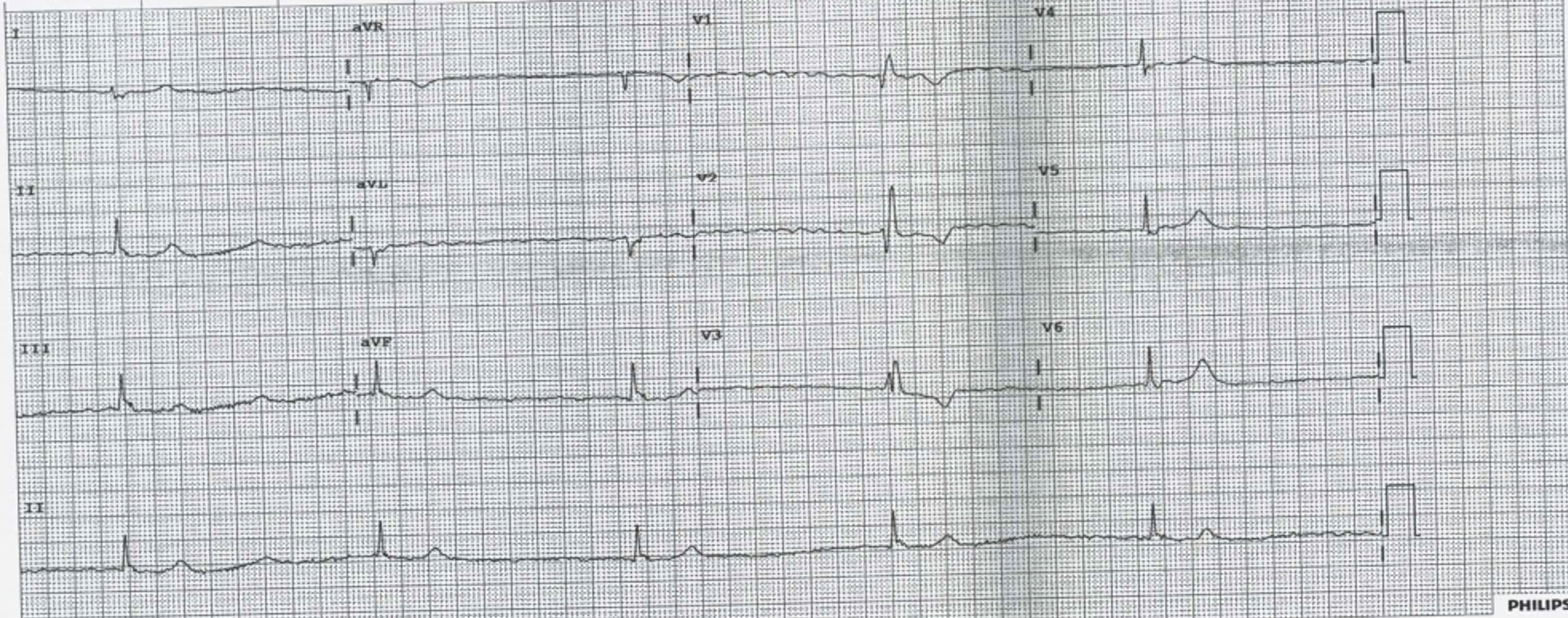
His ECG is shown below. After looking at his ECG, what would you do?
(a) Increase his heart rate using pharmacology
(b) Do nothing as you might cause harm and his BP is acceptable and he is alert.
(c) Defibrillate
(d) Give Magnesium or an extra dose of Sotalol
Beware assuming that this patient’s cardiac output is fine, given that he is alert and his blood pressure is ‘acceptable’. The cardiac output MUST be reduced. CO = HR x SV The only reason the blood pressure is not low is due to a sympathetic response mounted by the patients, resulting in increased vasoconstriction.
(a) Increase his heart rate using pharmacology- The only real answer
(b) Do nothing as you might cause harm and his BP is acceptable and he is alert. X the patients cardiac output is reduced and they are only perfusing due to endogenous sympathetic response.
(c) Defibrillate X
(d) Give Magnesium or an extra dose of Sotalol X
Pharmacological Increases in Heart Rate
ATROPINE
Muscurinic Acetylcholine Receptor Antagonist
t1/2 = 3-4 hours
Indication: AV nodal blockade. It works by decreasing vagal tone, so may not be effective in high degree AVN block.
Dose: Start at 0.5 mg-1mg (max of 3mg) Lower doses may cause a reflex bradycardia
Beware:
- Patients with coronary artery disease as can increase myocardial demand
- Acute angle closure glaucoma
- Bowel obstruction
- Cardiac transplant patients- may result in asystole.
Atropine may be the first line to use whilst you are getting set up for the definitive drug ie Isoprenaline. Atopine may not work on all patients or if it does work, beware, as it can wear off fairly rapidly.
ISOPRENALINE
Beta adrenoreceptor agonist
t1/2 = 5 minutes, but immediate onset of action
Dose: If given centrally start at 0.5-1 mcg/min and titrate. It is also safe for peripheral infusion and can be started at 5mcg/min then titrate up or down. Usual range is 2-10 mag/min, however higher doses have been used.
Beware: Hypotension, tachycardia, angina. May not be tolerated by the patient longer term as can cause headaches and trembling.
ADRENALINE
Non-selective adrenergic agonist Beta 1 > alpha 1 and Beta 2
t1/2 = 5 minutes. Acts within a minute and lasts for 5-10 minutes.
Dose: This can be used peripherally. Start dose at 1 mcg/min. Usual dose is 1-10 mcg/min. Higher doses may be needed.
It has a wide range of effect, being a chronotrope and inotrope.
Beware: Tachycardia and arrhythmias, narrow angle glaucoma, Phaeochromocytoma
What happened to the patient?









May be a trial of stopping Sotalol before considering pacing..??
Always stop I agree. Although the half life of Sotalol is about 15 hours…….. A long time to wait
checking potassium and renal function may reveal hyperkalemia as a cause of bradycardia….
I agree. I go further and say I check potassium in any patient that comes in with an arrhythmia. I have been surprised many times.
Are there flutter waves in V1?
Simon, I agree that they look a bit fluttery (if that’s a word), but they are in other leads. The only reason I haven’t paid as much attention to them is that the rate is so high. They are way above 300. I think they are just that fluttery look you get in these AF ecgs