A 27 yo 34/40 gestation G1P0 patient presented to the Emergency Department with central chest pain, with some radiation to between the scapulae. There was no shortness of breath or diaphoresis, nausea or vomiting or palpitations. The patient did not complain of leg pain. The registrar presented the case to me with the following findings.
Examination
- Vitals: HR 94, BP 120/85-140/90(variable), respiratory rate of 18 and sats of 96% on room air
- Chest was clear
- Heart sounds dual and no extra sounds
- Abdomen was soft
- Calves not tender.
- Bedside U/S showed a live foetus.
Lab tests
- FBC: Hb 119, WCC 8.4 PLT 103
- EUC: Na 139 K 4.5 Cr 44
- Troponin was 4 ng/L (ie., normal)
- D-Dimer 4.67 mg/L (<0.5)
An ECG was performed:
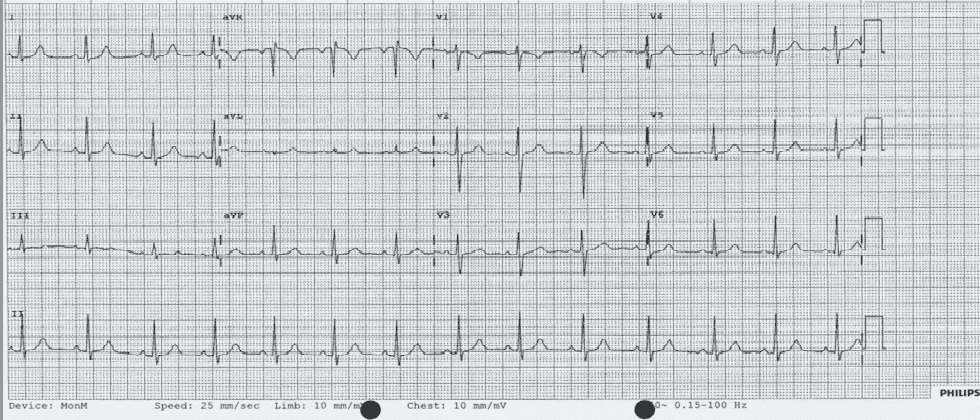
What would you do next?
(a) Serial Troponin
(b) Repeat ECG
(c) Ultrasound of the calves
(d) V/Q or CTPA
(e) Observe
What we did
The pain was very atypical and there was no troponin rise, although a big rise in D-dimer, the patient did not behave like a PE. Our approach was to observe and get a second opinion from the Medical unit.
The patient was observed in short stay and reviewed by the medical unit and discharged home. They did not believe that this was a PE.
What Happened Next?
The patient represented the next day with worsening chest pain that became worst on breathing. However this settled with simple analgesia in the emergency department. The patient also complained of epigastric pain.
Examination
- Vitals: HR 79, BP 130/90, Sats 98% on room air.
- Chest lear HS dual abdo soft, calves non tender
Labs
- FBC: Hb 110, WCC 8.0 PLT 79
- EUC: Na 137 K 3.9 Cr 44
- LFT: Bili 3 ALT 148 AST 141 ALP 108 GGT 23
- D-Dimer 8.38 mg/L (<0.5)
What would you do now?
(a) Admit for Observation
(b) Repeat troponins
(c) CTPA/VQ
(d) CXR
(e) Get urgent O&G Consult
What we did
- A Chest X-ray: There was no abnormality
- Doppler Ultrasound of the legs: No DVT above or below the knee
- Given that all this was normal we performed a CTPA shown
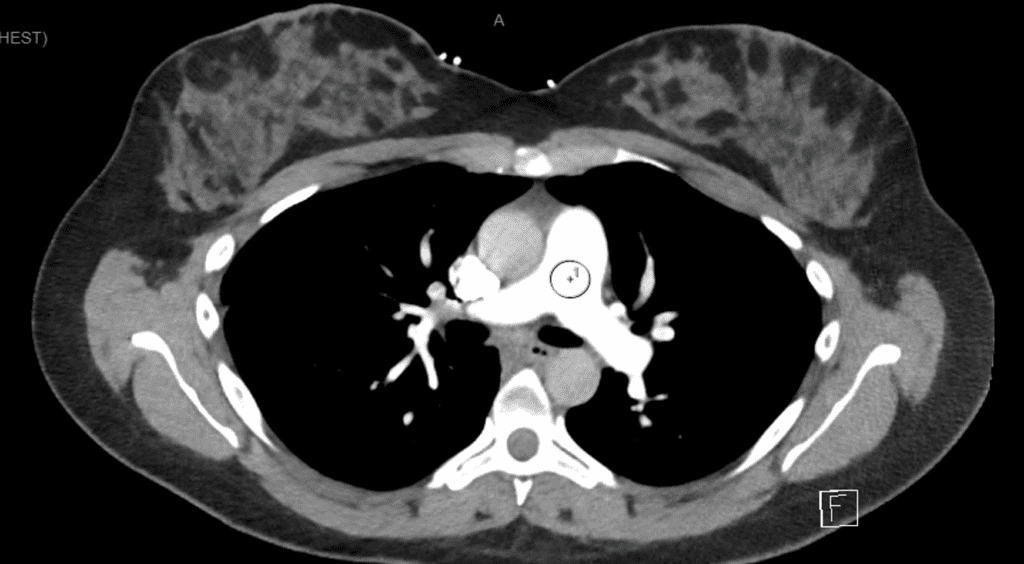
The patient was again reviewed and admitted to short stay unit for observation. Given a further ECG was normal and the CTPA was normal and the patient had no further pain, the patient was discharged.
Obsessive Compulsive Disorder is not always a bad thing……..
I obsessively follow up patients I have seen.
When reviewing this patient a few things stood out for me:
- The blood pressure had been 130/90
- The LFTs were a little deranged
- The patient had a low platelet count.
We recalled the patient.
The patient was well, however we repeated all the labs.
The patients blood pressure was 130/90, sometimes reading 140/90
- FBC: Hb 115, WCC 5.7 PLT 86
- EUC:Normal
- LFT: Bili 3 ALT 127 AST 77 ALP 122 GGT 31
- D-Dimer 7.79 mg/L (<0.5)
Putting it all together the concern was:
- Low platelet count
- Elevated liver enzymes
- Elevated Blood Pressure
Was this HELLP Syndrome?
The patient was admitted under the O&G team and observed for several days. A diagnosis of Gestational thrombocytopaenia was made and the patient discharged after a few days, for a planned delivery the following week.
HELLP Syndrome
It stands for HAEMOLYSIS, ELEVATED LIVER ENZYMES, LOW PLATELETS
- Up to 0.6% of all pregnancies,
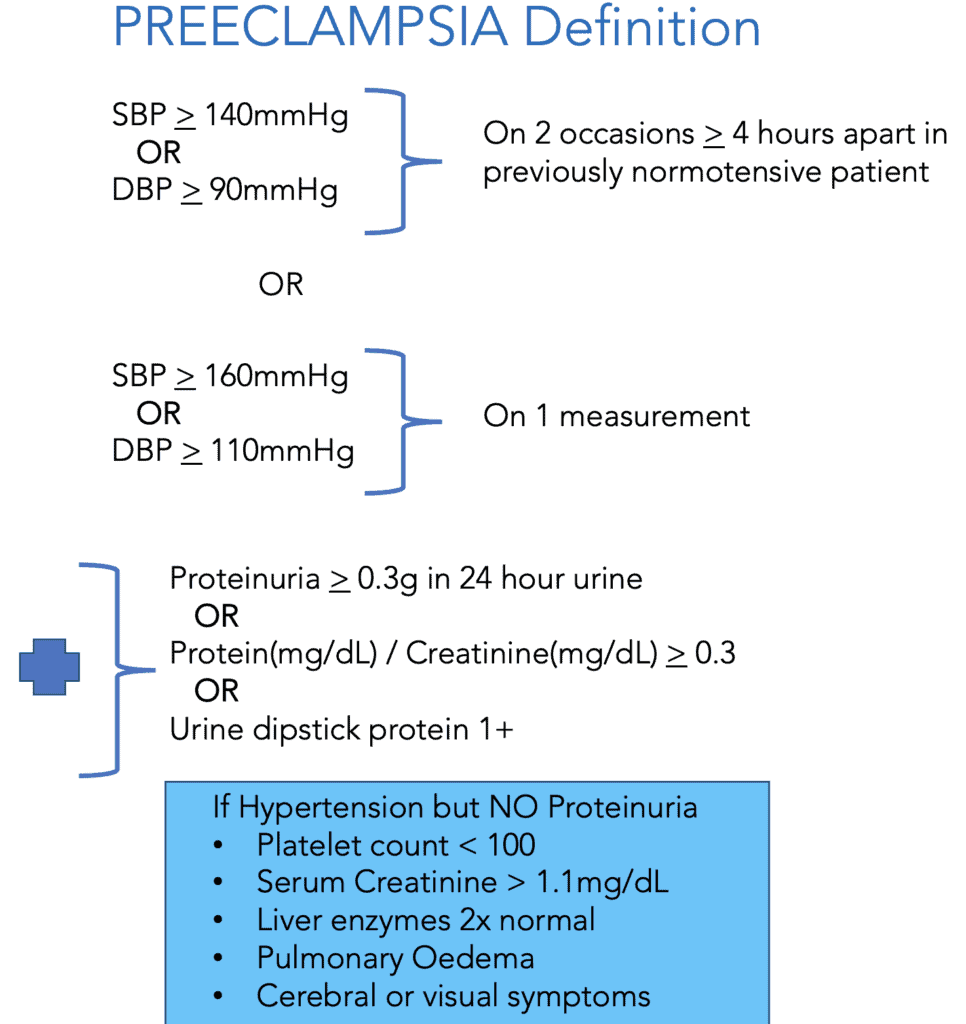
- Up to 12% of patients with preeclampsia (see below)
- It usually occurs in older maternal age patients
- It tends to occur in > 27 weeks gestation
- Up to 3% maternal mortality and significant morbidity including:
- Placental abruption(16%)
- Acute Renal failure (7%)
- Pulmonary Oedema(6%)
- DIC(20%)
- Associated with 9-24% fetal mortality from:
- placental abruption
- intrauterine asphyxia
- prematurity
Clinical Presentation
The History often includes: Nausea and Vomiting, Epigastric/Abdominal Pain, dyspnoea and oedema
The EXAMINATION may show tachycardia, tachypnoea hypertension and signs of dehydration.
Investigations
- FBC- looking at haemolysis and thrombocytopaenia
- Blood Film- Shistocytes, helmet cells, burr cells
- COAGs
- Fibrinogen Levels- usually decreased
- D-Dimer- Usually increased due to fibrinolysis/DIC
- LFTs
- Increased ALT/AST
- Increased LDH
- Increased Bilirubin
- EUC
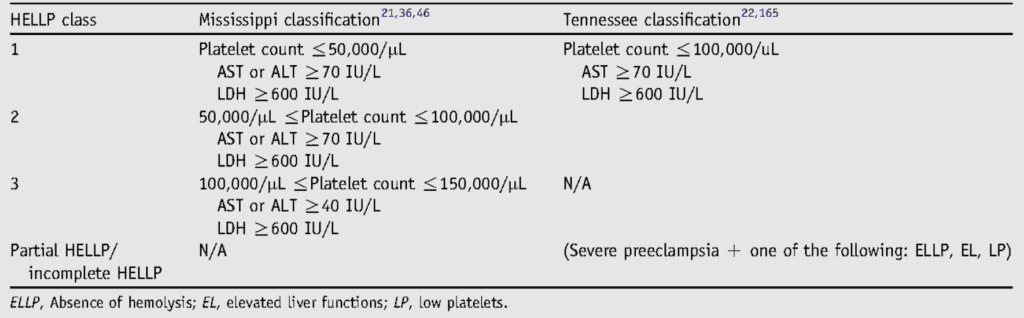
Classifications
There are two main classifications for HELLP that describe it’s severity.
MISSISSIPPI CLASSIFICATION: It divides HELLP into 3 classes based on platelets, AST, ALT and LDH. Class I is most severe.
TENNESSEE CLASSIFICATION: Describes HELLP as complete or partial. The partial classification includes:
- ELLP: Elevated liver enzymes and thrombocytopenia, but no haemolysis
- EL: Elevated liver enzymes.
- LP: Thrombocytopaenia
- HEL: Haemolysis and liver dysfunction
Management
- IV fluids
- Seizure Prophylaxis
- IV Magnesium Sulphate until 24 hours after delivery
- 6g loading over 20 minutes
- 2g/hr maintenance
- IV Magnesium Sulphate until 24 hours after delivery
- Blood Pressure Control
- Use Labetalol or Hydralazine
- Aim for SBP < 160 and DBP < 105
- Delivery or Steroids
- At > 34 weeks amn unstable=delivery
- At 24-34 weeks and stable= stable then steroids and plan
Potential Complications
Maternal:
- DIC, bleeding and haemolysis
- Pulmonary oedema, PE
- Cardiac ischaemia and arrest
- Seizures
- Renal Failure
Neonatal:
- Thrombocytopaenia
- Intrauterine growth retardation and prematurity.








Great case.
Did anyone speak to her obstetrician rather than medical unit?
May have helped an unnecessary discharge
Hi Adam
Public patient.
The issue is that it wasn’t apparent in the first presentation. O&G has a standard response. I think they just text it electronically: “Treat her like you would any patient” Not sure what to do with that
Common things occur commonly. It seems that no consideration was given to this (initially) could have been reflux oesophagitis, and trial of Gaviscon +/- PPI might have been worthwhile.
Hi Phillip
In fact a ‘pink lady’ was given as the original working diagnosis was not cardiac or PE.
There was improvement.
This is a miss by us , as an Emergency Medicine speciality…
The correct diagnosis should`ve been up there in our initial presentation differential diagnosis..
Also..
Why we as an ED specialists referring to the Medical or even the O&G Specialists ???
This is a bread and butter for our Emergency Medicine Speciality..
We should’ve made or at least alert the in pt service to the diagnosis in the initial presentation and admit the pt under the O&G to do the rest of the in pt service treatment…
ED Specialists are the king of the differential diagnosis, not the medical, surgical, O&G etc…
We should make the diagnosis rather than relying on other speciality..
Hi Khalid
Thanks for the comment
That’s why this is such a good case, and why I put it up.
It shows our fixation.
I will also say, it’s ‘bread and butter’ for everyone when presented on paper like this, but it’s not bread and butter when looking at it in real time. You know, you’ve had patients like that.
During the last EMCORE in Sydney we looked at a real time case of cervical injury in a child. Everyone could tell you what an approach might be on paper, but when the real-life issues got in the way, it wasn’t that easy, in a room full of emergency phsysians. That’s why it’s important to go over the case.
We were fixated on the D-dimer. It was so high. The patient did not behave like a PE, nor had any Troponin leak. In fact if not for the D-dimer, I wouldn’t have though of PE as high in the diagnosis.
I’ll fill in some of the story.
Patient presented to me by registrar and I did not think this was not a PE. We talked about the D-dimer as if we applied YEARS a CTPA would have been done.
I did not think it was PE and the Platelets were just a little low, LFTs normal and Trop normal and ECG normal and there was only one reading of a highish blood pressure. No more, so we can’t make the diagnosis of HELLP.
O&G were consulted who said no, just treat like you would any other patient…….thankyou
Instead of going in for a CTPA and exposing the patient to radiation ( remember the CTPA was negative anyway),given that my pre-test probability was low, it was decided to get another opinion.
It’s easy to just shoot off a CT. It’s hard to practice clinical judgement.
The problem here is the Medical team were asked to give us an opinion on PE.
They said no- BUT then NOTHING happened. The patient was discharged by the short stay reg. The fixation was on the darn D-dimer and the question of “Was it a PE?”. But we know this should not a binary question. We did not answer the question of “What was it?”
It shows that sometimes checking processes help. You will be surprised at how many abnormal ECGs I find and missed CT diagnoses, when I do my regular weekly check.
At EMCORE on the Gold Coast in January 2022, we will do several real-time cases like this where we as a group try to solve the riddle.
Keep going.
Thanks for the interaction.
I’m approaching 60(from the wrong side) and still learning.
Peter
i thought of dissection initially , where pregnancy is a predisposing factor…with the elevated Dimer still I have to think even more of dissection….
4 months ago I ve missed exactly same case ….with significant chest pain , the severity of which distract our attention away from preeclampsia and HELLP….
Still the question is : why there is chest pain of that severity in your and my case?? , I donot think simple reflux will cause a significant chest pain tat warrants more investigations on the part of any ER physician…If I will of reflux !! may be .. she is pimigravida with no much of previous pregnancy experience…(which is by the way is exactly the same in my patient …also was primigravida)…
if you are around 60 …I am 66 and still learning
Learning every day. However don’t be hard on yourself. I say there is a difference between paper medicine and real clinical medicine. In paper medicine, it’s simple, draw up an algorithm and fit everything into it, but we’re not trained chimps. The real physician will not find it so easy. Paper medicine isn’t real. There will be nuances and gestalt and concerns and twists and turns. This year at EMCORE I am conducting a live panel discussion of this case. When we are finished in January, I will put it up and you can see that nothing is straight-forward. You will see how many disagree and how differing the approaches are. PE is still an art form.
Every time I teach, I learn and every-time I learn, I teach!
Keep learning and teaching.
Peter
Great case, Peter.
I am wondering re: imaging pathway for evaluation of PE in pregnancy.
We use YEARS algorithm as well but it usually recommends CTPA.
Based on WA and NSW PE evaluation pathway, start with D-dimer, and then CXR to choose between VQ scan and CTPA. No VQ or CTPA if lower limb DVT U/S positive.
If normal CXR and then get V/Q scan ( perfusion scan initially ).
CTPA if V/Q scan indeterminate.
You did CTPA In this case. Is it due to the availablilty or your preference ?
I really appreciate for sharing the case for learning.
Hi Aung
Thankyou for reading.
PE in pregnancy is always tricky.
In terms of radiation as you know, we want to avoid radiating breast tissue and radiating the foetus, mostly to reduce the risk of breast Ca in the mother and leukaemia un the newborn. However the dose of radiation in a CTPA is lower than the dose required to cause this disease(but is cumulative).
I’ve never been sure of the use of ultrasound. We know that we miss up to 30% of below knee, in this aerator-dependant procedure.
The use of CXR makes some sense, if we are looking for something in the chest X-ray. In terms of VQ scan we do the CXR to look for an abnormality that will stop us from doing a VQ. However this group of patients is a very young group and with no previous history, it is extremely rare to find an abnormality in the CXR. The concern is in that small group where the VQ comes back negative and we have to add a CTPA.
It is easier and faster and leads to potentially even less radiation if we just go to CTPA, plus we can uncover other abnormalities.
Currently there are about 7 guidelines out there. These guidelines show the lack of agreement. For example:
In terms of leg U/S, 2 guidelines don’t recommend it and 3 do, but only if there is leg pain. I agree, if there is no leg pain, why do it, the yield is so small.
VQ I think is fine in this young population and reducing the radiation dose is possible. One thing to say about thVQ and CTPA, is that there is no consensus on what the radiation doses emitted are.
I like CTPA as it’s readily available(overnight as well, which VQ is not in most cases), gives us all that we need and looks for other things and we can use shielding to reduce the dose even further. Also in about 5% where a VQ is indeterminate, we will CTPA and increase the radiation dose significantly.
This year at EMCORE on the Gold Coast in January(www.emcore.com.au), I will hold a live panel discussion on this case and see what experts say. I will try and put that video up when it’s done.
Peter