Here are some examples.
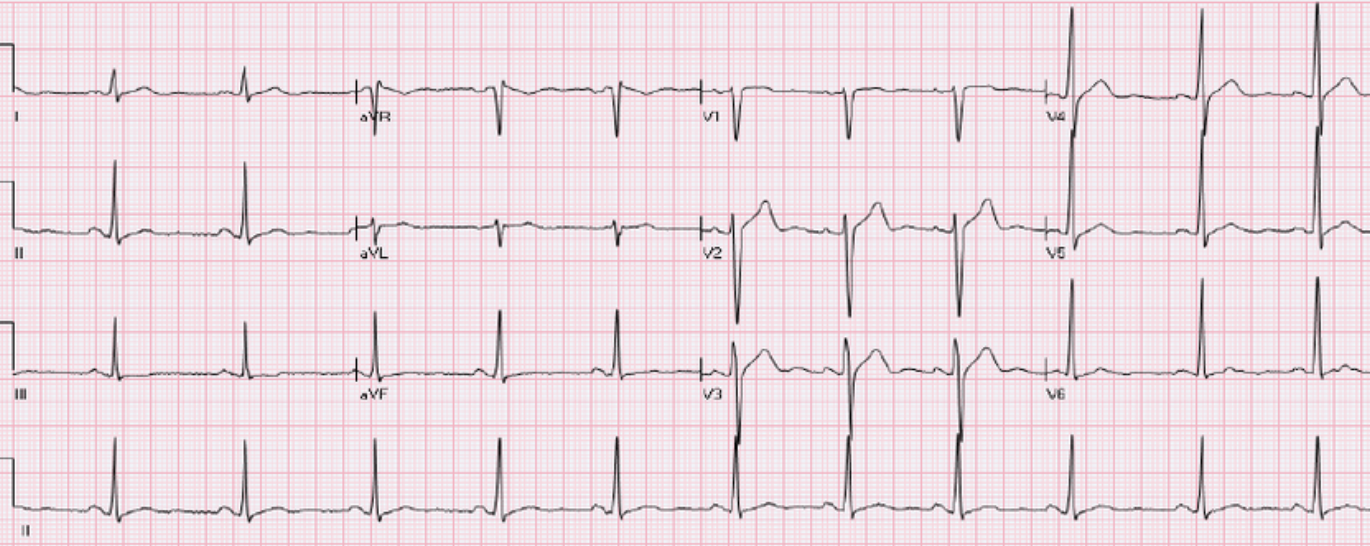
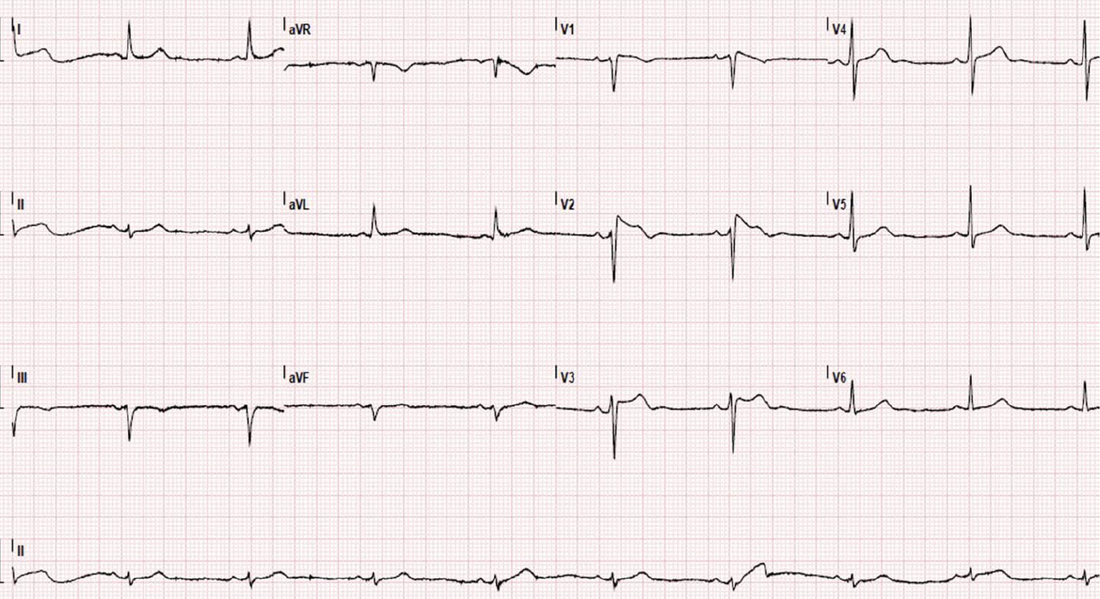
1. Normal ST Elevation
This can be in 2 forms, where in both the ST segment is concave:
- Male pattern: 1-3 mm STE in V1-V4
- Female pattern: 1mm STE in V1-V4
The formal definition of a STEMI as per AHA/ACC(2) is:
- Men
- < 40 yo: >2.5 mm ST-elevation in V2 or V3, 1 mm in any other lead
- > 40 yo: >2.0 mm ST-elevation in V2 or V3, 1 mm in any other lead
- Women: >1.5 mm ST-elevation in V2 or V3, 1 mm in any other lead
The ECG below is from a male who presents with chest pain. It is normal.
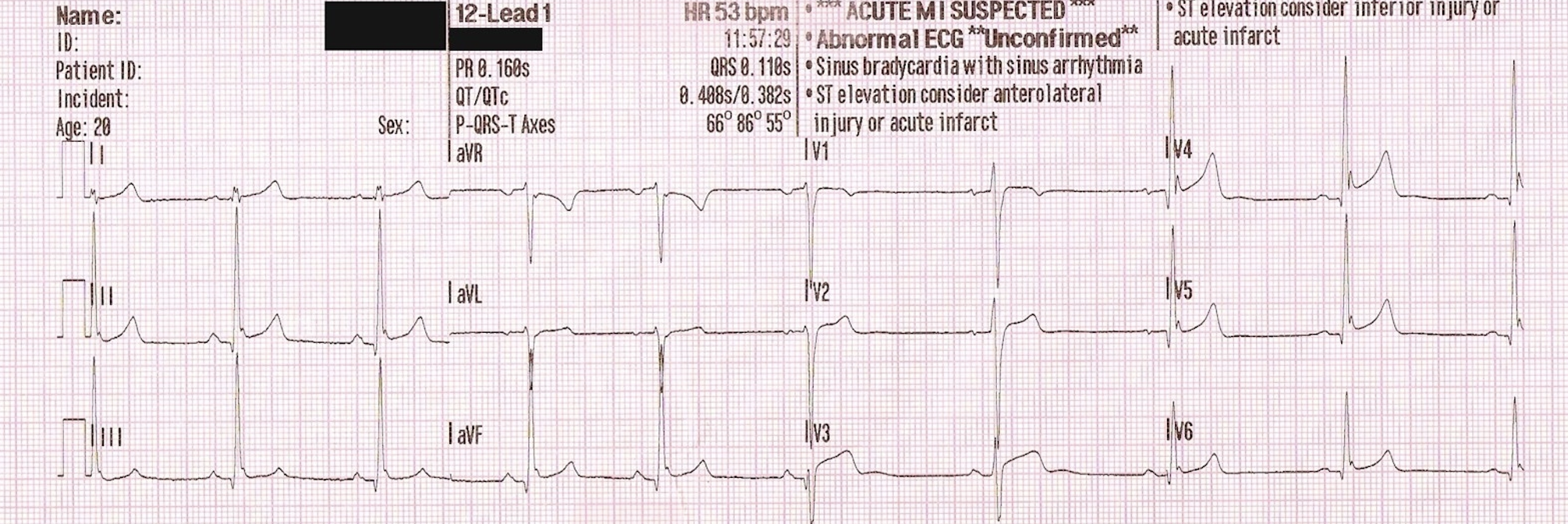
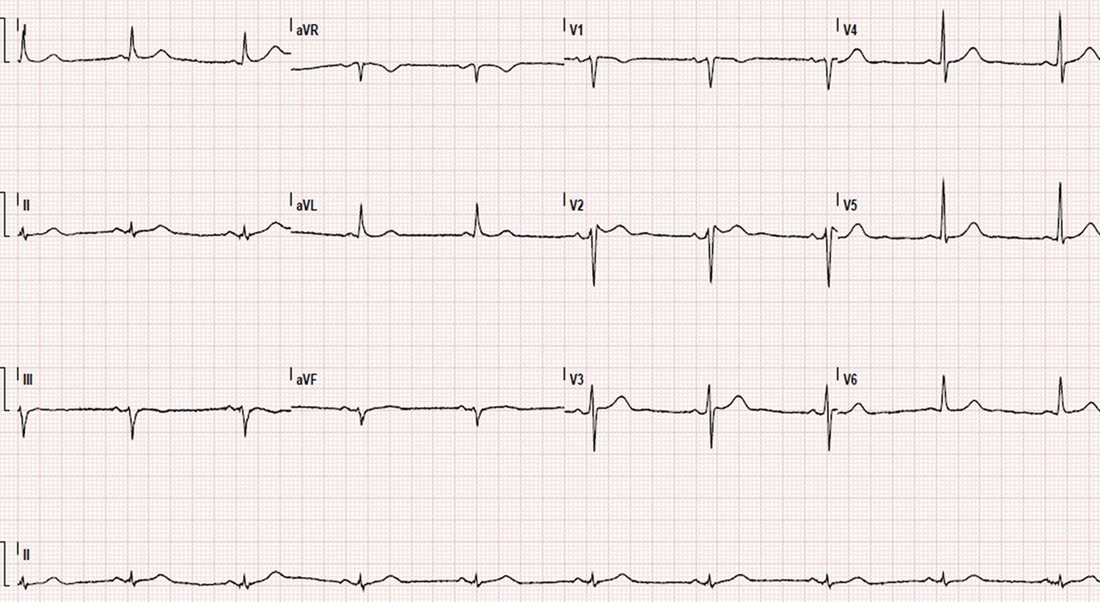
2. Benign Early Repolarisation (BER)
This condition is present in a younger population group and amongst athletes. There are three types:
- Type 1: Pattern occurs in the lateral leads
- Type 2: Pattern occurs in the inferior/inferolateral leads
- Type 3: Pattern occurs throughout the whole ECG.
BER Pattern:
Point notch with elevation
STE with concave up morphology V2-V6, II, III, avF usually < 2mm
No reciprocal changes
Symmetrical Concordant T wave
STE/T-wave height <0.25 in V6
Benign Early Repolarisation may not be that benign, being associated with serious arrhythmias in some studies.
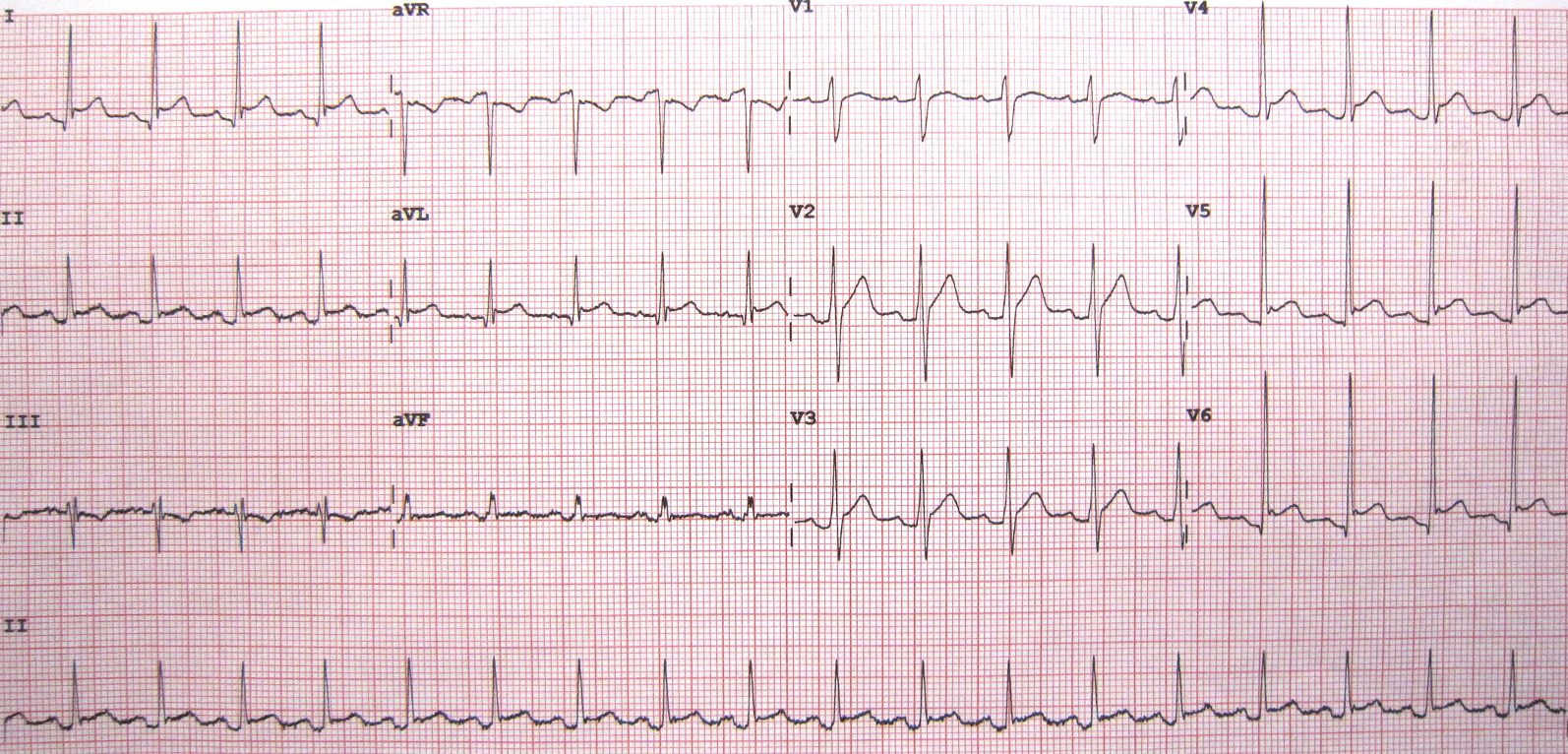
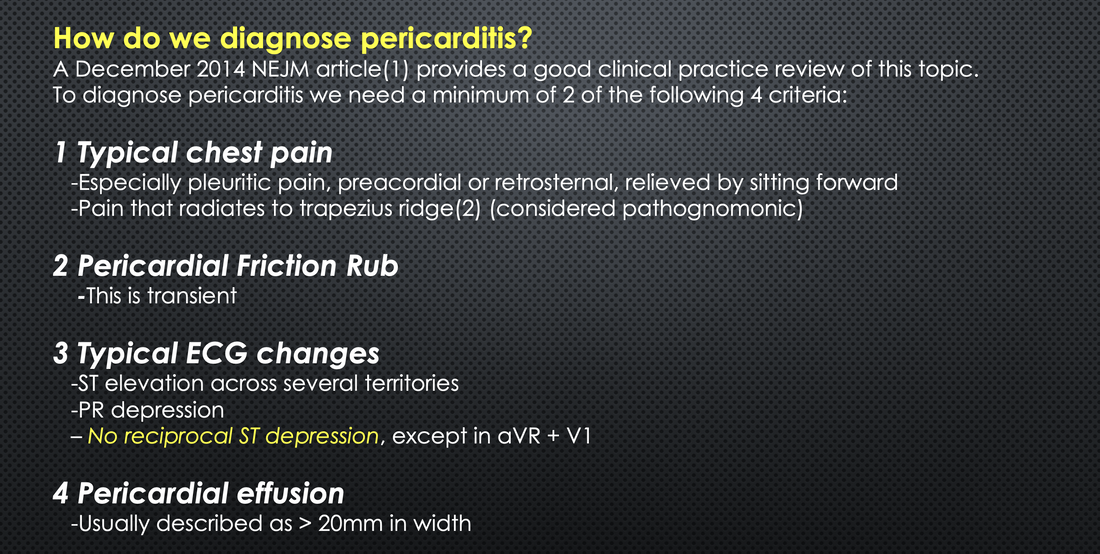
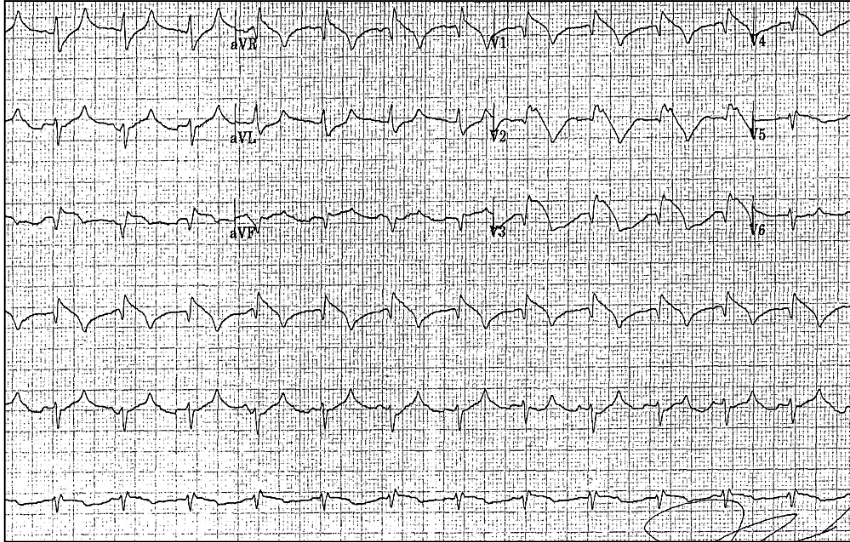
3. Pericarditis
Diffuse STE
ST/T-wave >0.25
There are 4 stages in pericarditis:
- Stage I: ST and PR changes
- Diffuse concave up ST segment elevation,
- Reciprocal ST depression in aVR.
- PR elevation in lead AVR + V1
- Stage II: Normalisation of ST segments
- Stage III: T wave inversions.
- Stage IV: Normalisation of T waves
4. LBBB
STE is concave and <5mm
5. Hyperkalaemia
Downsloping ST segment.
6. Brugada Syndrome
Type I: Coved Pattern
- Leads V1-V2
- High take-off > 2mm and concave downscoping ST segment
Type II: Saddle-back
- Leads V1-V2
- Minimum ST elevation
7. Pulmonary Embolism
Can present with STE in Precordial leads
A more common presentation of right ventricular injury is STE in V1-V3 and/or ST depression of V4-V6.
Theories for why STE occurs in the precordial leads include:
- Paradoxical Embolism via atrial-septal defect or patent foramen ovale (5)
- Myocardial ischaemia caused by a sudden pressure load on the right ventricle, which is unable to compensate.(5)
- Hyperaemia from PE induces a catecholamine surge, increasing myocardial workload and ischaemia.(6)
References
- Wang K, et al. ST- segment elevation in conditions other than acute myocardial infarction. N Engl J Med. 2003 Nov 27; 349(22): 2128- 35.
- O’gara PT, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):e362-425.
- Kayanı WT et al. ST Elevation: Telling Pathology from the Benign Patterns. Global Journal of Health Science. May 2012, 4(3):51-63
- Mirijello A et al. Brugada electrocardiographic findings in an 80-year-old man. BMJ Case Reports. July 2013.
- Cheng TO. Mechanism of ST-elevation in acute pulmonary embolism. Int J Cardiol. 2005;103:221-223
- Falterman TJ, et al. Pulmonary embolism with ST segment elevation in leads V1 to V4: case report and review of the literature regarding electrocardiographic changes in acute pulmonary embolism. J Emerg Med. 2001;21:255-261.
- Wilson G T et al. Pulmonary Embolism Mimicking Anteroseptal Acute Myocardial Infarction. JAOA • Vol 108 • No 7 • July 2008







