This week’s teaching is based on the new ACS guidelines. We will be concentrating on ECGs and STEMI Equivalents.
Here are the STEMI equivalents proposed in the guidelines.

This week’s teaching is based on the new ACS guidelines. We will be concentrating on ECGs and STEMI Equivalents.
Here are the STEMI equivalents proposed in the guidelines.
In this weeks teaching we looked at the approach to the comatose Post ROSC patient.
Some key learning included:
Post ROSC patient care is a continuation of resuscitation. We must concentrate our efforts as intensely in the post ROSC period as we do, during the initial resuscitation to obtain ROSC.
During the initial resuscitation our goal is to DETECT OUTPUT. Post ROSC, our goal is to measure and control everything as much as possible, to ensure the best survival rates.
Ischaemic injury occurs early in resuscitation, ie in the first few minutes of anoxia. In the emergency setting, as well as during reperfusion. In the post ROSC comatose patient, it is difficult to determine a prognosis for good neurological survival in the emergency department. This is done > 48 hours following ROSC.
In the post ROSC comatose patient, we should aim for the following:
Blood Pressure:
Oxygenation and Ventilation
Temperature Control
Seizures
An Approach to the Dizzy Patient:
 Here are 4 cases to consider. Come up with a diagnosis for each.
Here are 4 cases to consider. Come up with a diagnosis for each.
Case 1: A 68 yo woman presents with dizzyness, that was sudden in onset and she collapsed to the ground, but did not lose consciousness. She often has ringing in her ears and has reduced hearing loss on the right side. She has not been investigated for this. What is your working diagnosis and what would you do next?
Case 2: A 78 yo woman presents with dizzyness. She has had several episodes over the last 2 months, but more frequently over the last week. Symptoms have now resolved and her examination is normal. What is your differential diagnosis?
Case 3: A 68 yo male presents with a sudden onset of dizziness. The room is spinning. He tries to sit up in bed, for an examination, but cannot. What is your working diagnosis?
Case 4: A 48 yo woman presents with 9 months of constant dizziness. She has had an MRI scan 8 months ago which was normal. She is now complaining of left arm weakness. When you test the pronator drift sign, she raises both arms up to the level of her shoulders and the left arm lowers as in the image below. What is your diagnosis?

At our next teaching session we will be discussing ‘The Patient with Syncope’. Although the ECG only has a yield of about 5%, it is the most important investigation we will perform in patients with syncope.
Click this link to go to an ECG Quiz. Click on the ECG quiz at the top of the page. Here you will find 9 important ecgs to review. They are the ECGs of Syncope.
Please complete prior to the next teaching session.
Watch the Video if you missed the teaching, or watch and review.
A 26 year old mechanic is brought in by ambulance after an overdose of an unknown substance. On arrival his vital signs are:
HR 106, BP 80/50, GCS 12 sats 100% on RA, RR 34
An arterial blood gas drawn on arrival is shown below.
Describe and interpret the results.
FiO2 0.21
pH 7.15
pO2 115 mmHg
pCO2 20 mmHg
HCO3 8 mmol/L
BE -16
Na 135 mmol/L
K 6.5 mmol/L
Cl 95 mmol/L
Glucose 6.2 mmol/L
Urea 8.1 mmol/L
Lactate 5.2 mmol/L
measured osmolality! 320 mosm/Kg
1) Acid-Base Balance
Severe acidaemia (7.15)
Moderate hypocapnoea
respiratory alkalosis
Severely low HCO3 and large -ve BE
metabolic acidosis
expect CO2 for HCO3 8 = 8 + 1.5 x 8 = 20mmHg
.: diagnose appropriate respiratory compensation
AG = 135 – 95 – 8 = 32
Delta ratio = (32 – 16)/(24 – 8) = 16/16 = 1.0
.: diagnose isolated RAGMA
Therefore Dx RAGMA with appropriate resp compensation
2) Oxygenation
Mild hyperoxaemia on room air
A-a grad = 150 – 1.25×20 – 100 = 150 – 25 – 100 = 25
Expect Aa 20yo = 20/4 + 4 = 8
.: Dx mildy raised Aa grad, implies V/Q mismatch
3) Electrolytes
Normonatraemia
Hyperkalaemia
expect K+ for pH 7.15 = 5 + 2.5 x 0.5 = 5 + 1.25 = 6.25mmol/L
.: K+ 6.5 is appropriate for pH
Mild hypochloraemia
electrical equilibration RAGMA
Normoglycaemia
not cause ALOC
Significant hyperlactataemia
Hyperosmolar state: risk cerebral oedema
osmolar gap = osmc – osmm
= 320 – (2 x Na + urea + glucose)
= 320 – 270 – 8 – 6
= 50 – 14 = 36 ie high
STRONGLY implies toxic alcohol ingestion! ! ! check urine for oxalate
check formic acid levels
4) Interpret
Overdose, young man, severe metabolic compromise
compensated RAGMA plus raised osm gap
suggests ethylene glycol or methanol intoxication
haemodialysis likely indicated: consult ICU
needs paracetamol level (coingestant)
evaluate for other causes of lactate: septic screen, GI bleed etc
Please think about this case and answer the following questions for yourselves. We will cover them in the teaching.
A 52 yo presents with 2 days of increasing SOB and chest pain.
At rriage the sats are 62% on room air and the BP is 85/40
The patient is sent straight to a resus cubicle.
Monitoring and a non-rebreather mask is applied. An IV is inserted and pathology taken. Non-nvasive ventilation is prepared.
The patients blood gas and ECG are shown below. Please think about these and interpret them. If you are having trouble with them I have included some references on this website that you can look at to help you. Scroll down for the rest of the case.

The patient’s ECG is shown below. Please think about this ECG and interpret.

Case Continued:
You cannot get any assistance in the Emergency Department and are the senior doctor on, ie., there is no MET call:
This patient then becomes unresponsive. What do you do now?
Think about how you would approach this resuscitation.
Below some references to help you with the Gas and the ECG.
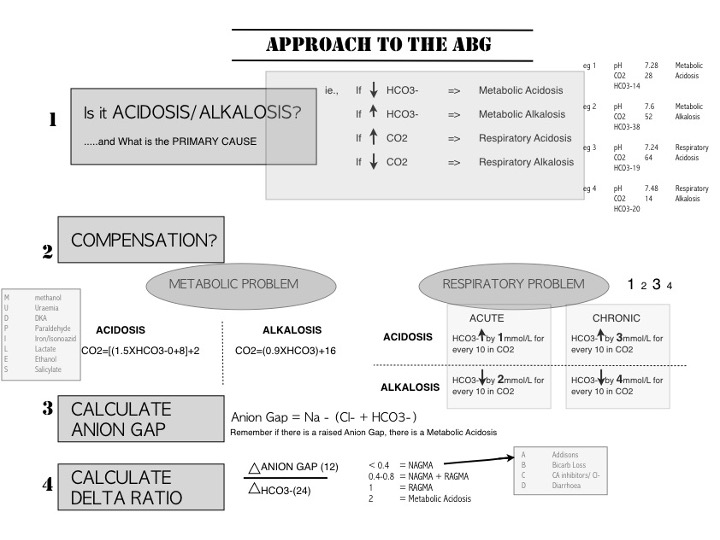
Below is an infographic I have put together for you, so you can use for future gas interpretation. I will be asking you all to interpret gases in the emergency department. Please use this. Remember you won’t learn this all at once, but this will for a basis for what we keep doing. Keep it on your phone.
OKAY A big few days for you and a bit of learning.