Introduction
This review is based on a great journal article just published (1)
The most common hip dislocation is a Posterior Dislocation
The most common Cause of a posterior hip dislocation is:
- In Native Hips: Motor vehicle accidents
- In Prosthetic Hips: Bending over, although they are much easier to dislocate from any movement
The most common complication of a dislocation:
- Sciatic Nerve injury-occurs in about 20% (2)
Our greatest concern associated with a hip dislocation:
- Femoral Head Necrosis (3)
- 5% incidence if reduced in < 6hours
- 53% incidence if reduced in > 6 hours
Clinical Presentation
The affected leg is shortened and internally rotated. It may be held in adduction.
Reduction Techniques
There are many reduction techniques, shown in the feature article and in the literature. Some of the techniques require flexibility, dare I say even contortion by the clinician. They may be too difficult to use. My aim here is to choose the easiest techniques to apply.
Remember the keys to reduction:
- Stabilisation of the pelvis, so it doesn’t lift when the technique is attempted
- Ensuring traction and axial force is at the hip and not at the knee (where injuries can occur)
Here are three of my favourite techniques:
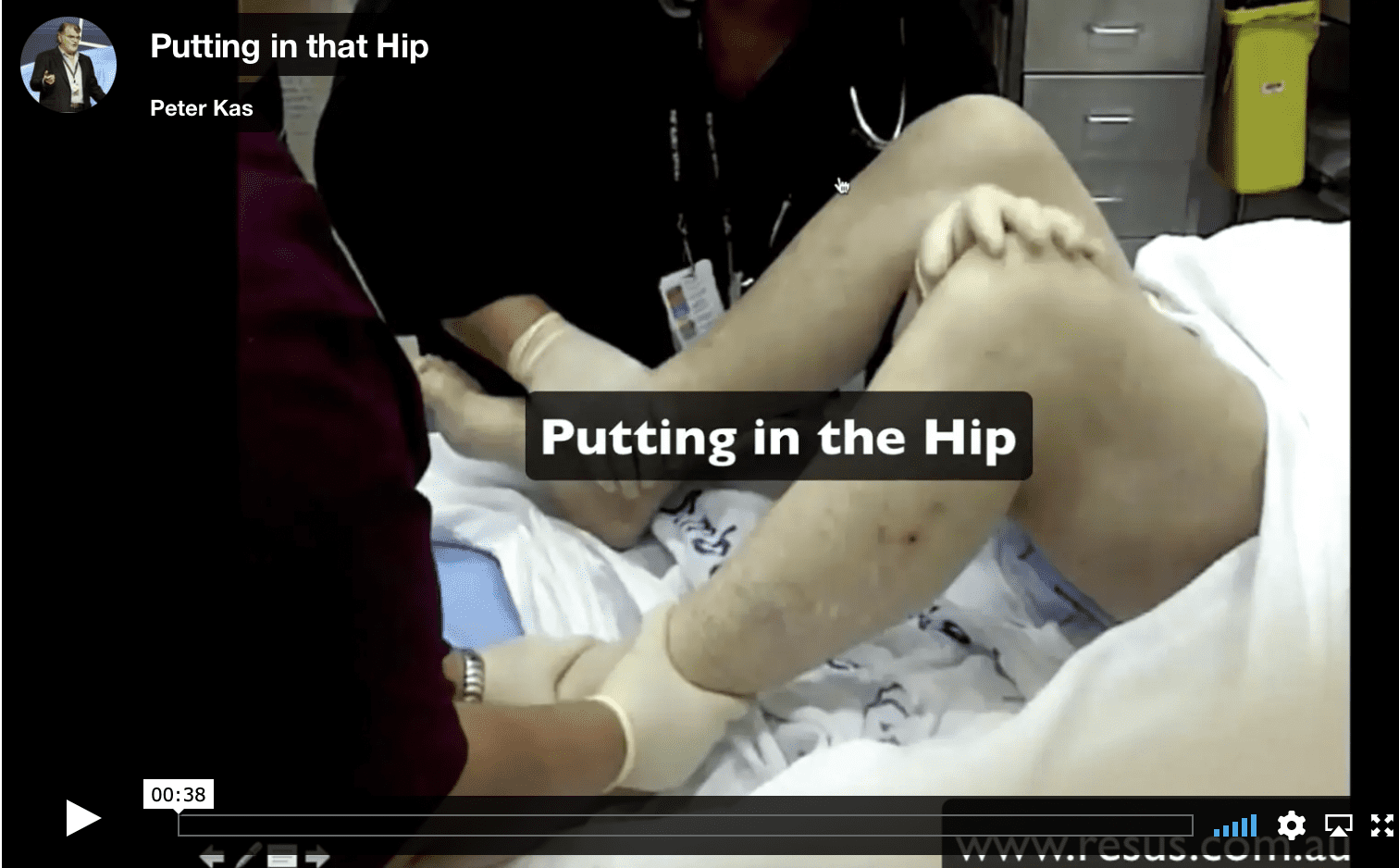
THE WHISTLER TECHNIQUE (4)
I sometimes call this the under-over technique. It’s my favourite technique.
- Both of the patient’s knees are flexed
- The ankle of the unaffected side is stabilized
- The clinician places their arm under the knee of the affected leg and over the normal knee, holding the normal knee.
- The clinical stands, putting traction on the hip joint
- The pelvis should be stabilised, to avoid the patient being lifted off the bed.
- Some gentle rotation of the leg may be needed.
- It has a 73% success rate.
See the video below:
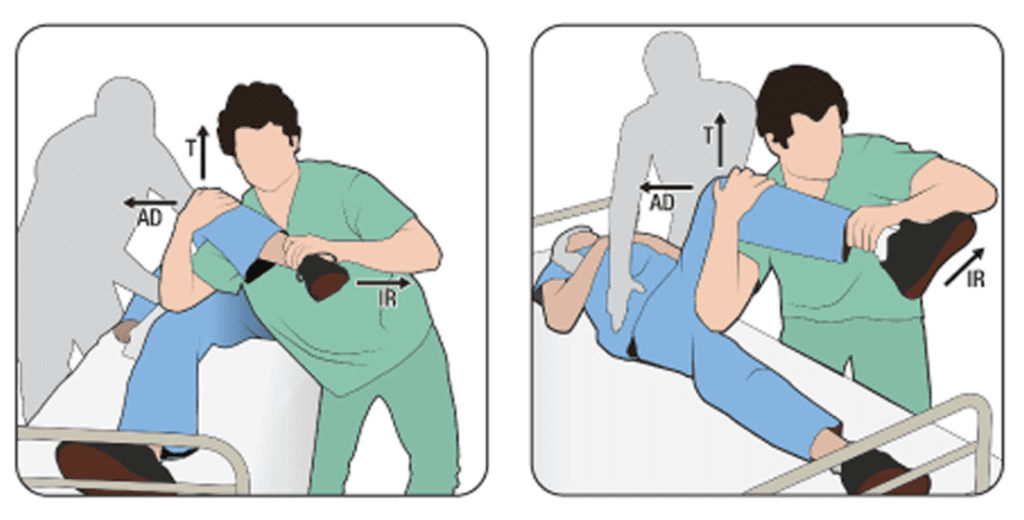
THE ROCKET LAUNCHER (5)
The first version of this that I saw, appeared quite dangerous for the patient. In that version, the clinical was at the end of the bed and the patient’s unaffected limb, hung off the end , with the other limb on the doctors shoulder.
A better form is the following:
- The affected hip and knee are flexed at 90 degrees
- The knee is placed over the clinicians shoulder
- The clinician then leans forward, which induces traction and then stands up.
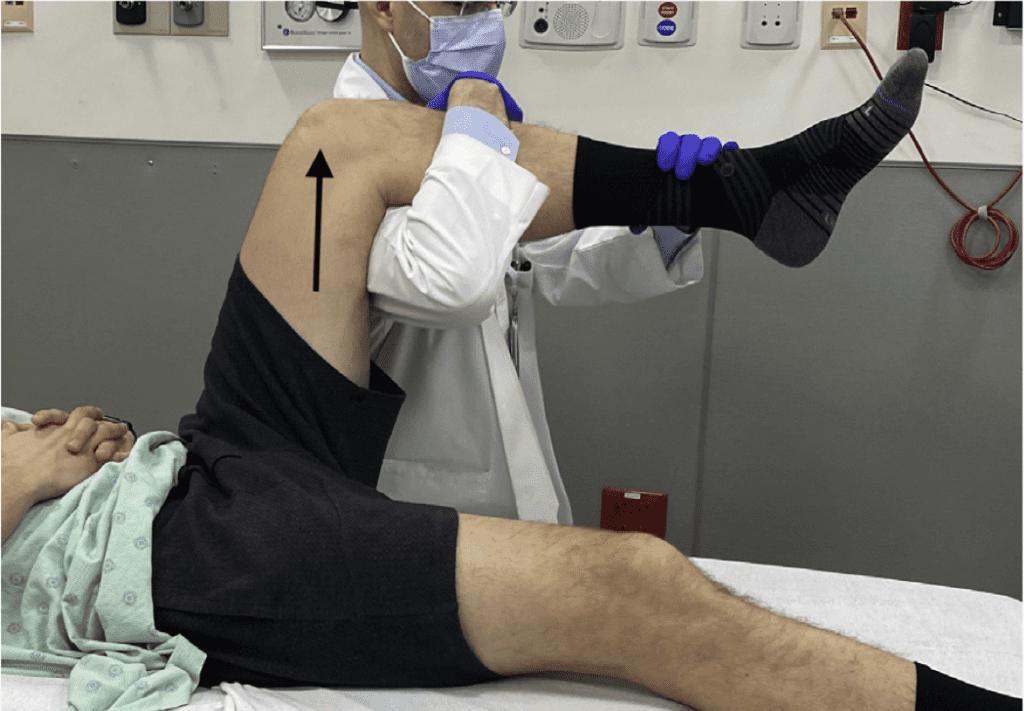
THE MODIFIED ALLIS (6)
This was the original technique I used, when I worked in a single doctor emergency department. I stood on the bed and the patient’s hip and knee were flexed at 90 degrees. I used to then pull upward on the leg, applying traction. It worked, but was potentially quite dangerous for me. I nearly came off the bed on several occasions.
This is a much better and safer version.
- The clinician stands on the side of the bed.
- The patient’s knee is placed over their shoulder. The patient may need to be angled on the bed for this to happen.
- The clinician stands applying the upward force.

References
- Gottlieb M. Managing Posterior Hip Dislocations. Ann Emerg Med. 2022 Jun;79(6):554-559.
- Hillyard RF, et al. Sciatic nerve injuries associated with traumatic posterior hip dislocations. Am J Emerg Med. 2003;21:545-548.
- Hougaard K, et al. Traumatic posterior dislocation of the hip– prognostic factors influencing the incidence of avascular necrosis of the femoral head. Arch Orthop Trauma Surg. 1986;106:32-35.
- Walden PD, et al. Whistler technique used to reduce traumatic dislocation of the hip in the emergency department setting. J Emerg Med. 1999;17:441-444.
- Dan M, et al. Rocket launcher: A novel reduction technique for posterior hip dislocations and review of current literature. Emerg Med Australas. 2015;27:192-195.
- Gottlieb M. Hip dislocations in the emergency department: a review of reduction techniques. J Emerg Med. 2018;54:339-347.







