A 52 yo male presents with atypical chest pain for 3-4 hours. He has had a vague feeling of chest heaviness for the whole day and has had an episode of palpitations. His only past medical history is of hypertension.
Examination is normal, with dual heart sounds and no reproducible chest pain on palpation. Lungs are clear and abdo is soft.
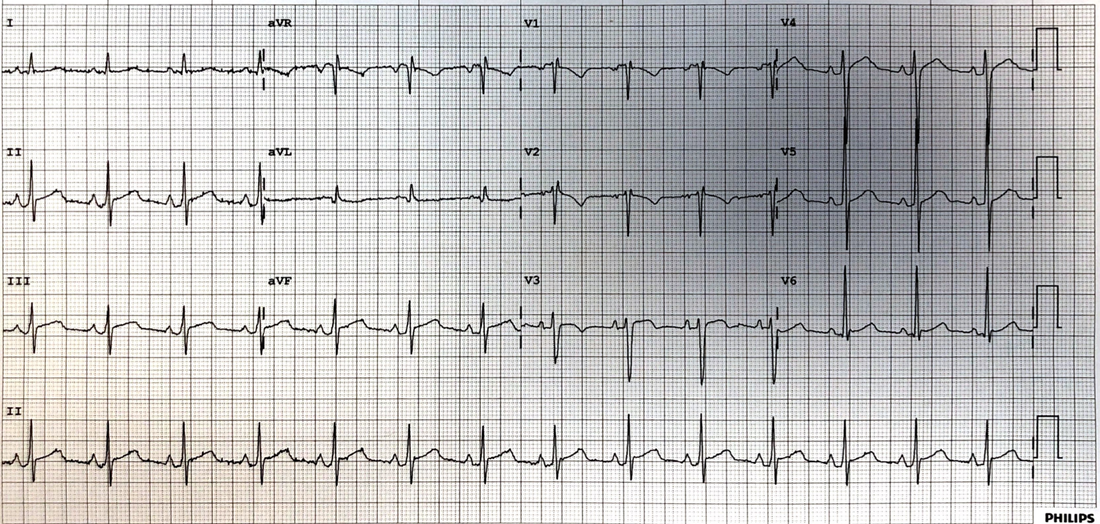
An ECG is done as shown below. Which of the following diagnoses does this represent?:
(a) STEMI
(b) Ischaemia
(c) Pericarditis
(d) Benign Early Repolarisation
Examination is normal, with dual heart sounds and no reproducible chest pain on palpation. Lungs are clear and abdo is soft.
An ECG is done as shown below. Which of the following diagnoses does this represent?:
(a) STEMI
(b) Ischaemia
(c) Pericarditis
(d) Benign Early Repolarisation
ANSWER
This is not a straightforward ECG, as few of them are. My diagnosis and the diagnosis we gave this patient was pericarditis. The patient did very well on standard pericarditis treatment.
Below is my thinking, plus also view the image below this:
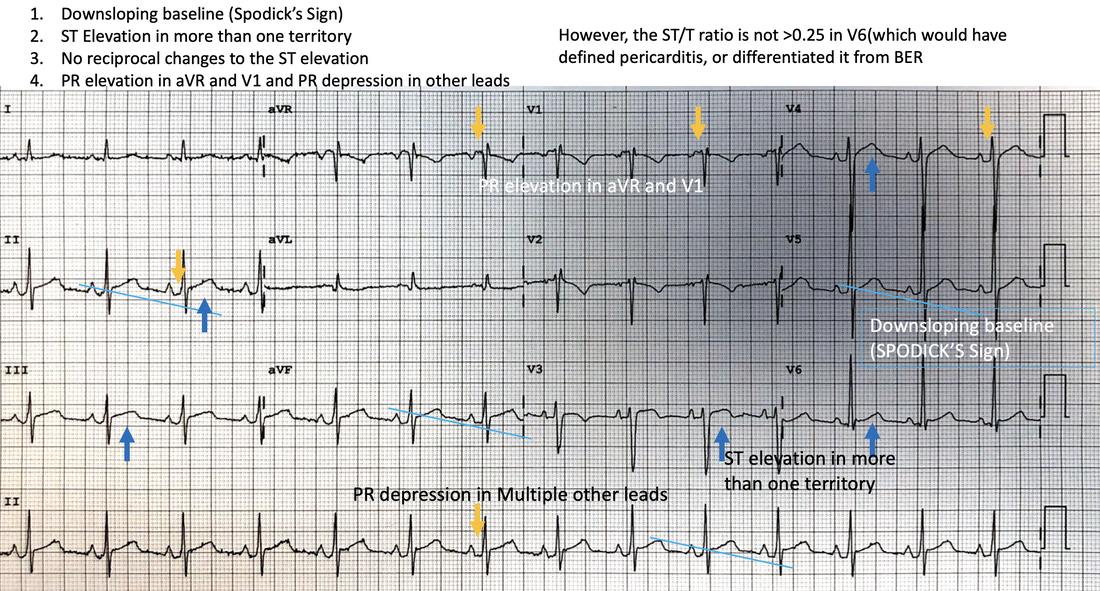
- It is not a STEMI and although there is ST elevation in multiple regions there are no reciprocal changes to be seen
- In terms of just plain ischaemia, there are very few changes here.
- The diagnosis of pericarditis is the most probable for the following reasons:
- There is ST elevation in multiple territories, with no reciprocal changes
- There is a down-sloping baseline, indicating Spodick’s Sign
- There is PR depression in several leads except aVR and V1 where we would expect pr elevation and it is present.
- The only thing not present which would have made it a ‘slam dunk’ diagnosis is that the ST/T ratio in V6 is not > 0.25
- It is not likely to be benign early repolarisation as there is no J point to be seen especially in V4