An excellent review article on Trigeminal Neuralgia, has just come out in the NEJM(1). Here is a quick summary.
FACTS
- Usually affects the mandibular or maxillary division of the Trigeminal Nerve
- F>M
- Right face > left.
- Bilateral is rare – look for other causes
CLINICAL PICTURE
Trigeminal Neuralgia is diagnosed clinically and must have 3 criteria:
- Pain in one or more divisions of the Trigeminal Nerve
- Sudden intense, short-lived electric-shock-like pain lasting seconds
- Up to half of patients describe constant pain between attacks, which is throbbing or burning.
- Pain is triggered by stimuli to the face or intraoral trigeminal territories
- Stimuli may be benign such as a breeze blowing across the face.
- Most patients will have trigger points. However the points and the position of manifestation of the pain can be different.
Clinical examination may reveal mild hypoesthesia, however, sensory abnormality is rarely found.
‘Tic Convulsif ‘ is a contraction of the facial muscles and may be seen during an attack.
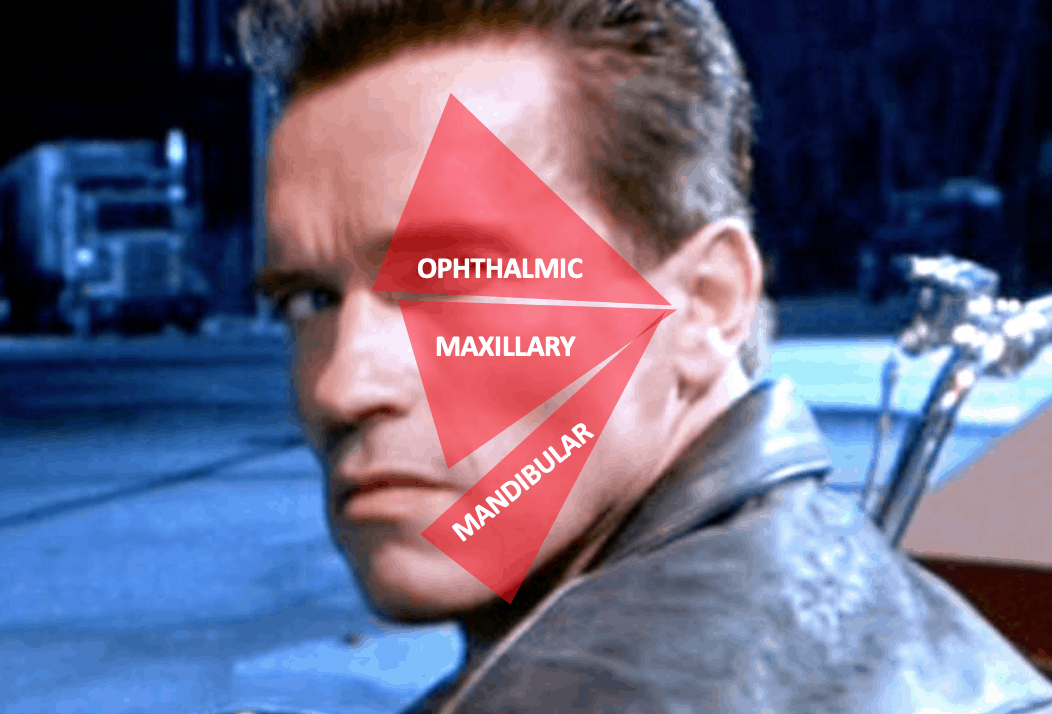
BASICS OF THE CN V
 3 divisions:
3 divisions:
- OPHTHALMIC
- Supplies the skin of the forehead, also the cornea and conjunctiva
- MAXILLARY
- Supplies the skin of the middle of the face and the mucous membranes of the upper part of the mouth, palate and nasopharynx
- MANDIBULAR
- Supplies the skin of the lower jaw and the mucous membranes of the lower part of the mouth
The Trigeminal Nerve has both Motor and Sensory Functions
- SENSORY FUNCTIONS
- Test all 3 divisions of the trigeminal for sensation
- The CORNEAL REFLEX: Touch the cornea with a sterile piece of cotton wool
- Both eyes should blink
- This is via CN VII(Orbicularis oculi)
- If only the contralateral eye blinks, there is ipsilateral CN VII palsy
- Ask the patient if they felt the touch on the cornea (CN V(1))
- Both eyes should blink
- MOTOR FUNCTIONS
- Temporal and Masseter muscles
- Feel the muscles
- Bite on a tongue depressor
- Try to open the mouth against resistance
- Unilateral lesion causes the jaw to deviate to the weak side
- Perform a jaw kerk
- Temporal and Masseter muscles
TYPES OF TRIGEMINAL NEURALGIA
Classical
- Most common
- Caused by intracranial vascular(usually superior cerebellar artery) compression of the sensory part of the trigeminal nerve root
- Anatomy is best seen with 3D, T2 weighted MRI
Secondary
- 15% of cases
- Due to a neurological disease
- Multiple sclerosis: risk of trigeminal neuralgia is increased by a factor of 20.
- Due to demyelination in the fascicle of the Trigeminal Nerve as it enters the ventral pons.
- Tumour at cerebellopontine angle
- Acoustic Neuroma
- Meningiomas
- Cholesteatomas and epidermoid cysts.
- Trigeminal neuropathies can develop secondary to
- Trauma damaging Trigeminal Nerve branches
- Facial trauma
- Dental procedures
- Rheumatological Diseases:
- SLE
- Scleroderma
- Idiopathic Trigeminal Neuropathy
- Benign, bilateral symmetric, purely sensory Trigeminal Neuropathy
- Facial onset sensory motor neuropathy
- May present as unilateral paroxysmal facial pain
- It is a serious and progressive disease.
- Trauma damaging Trigeminal Nerve branches
- Multiple sclerosis: risk of trigeminal neuralgia is increased by a factor of 20.
Idiopathic
- 10% of cases
MANAGEMENT
Medical
First choice regardless of cause of pain:
- Carbamazepine 200-1200mg per day or
- Side effects may include dizziness, diplopia and ataxia.
- Oxcarbazepine 300-1800mg per day
They work as Na channel blockers.
Gabapentin, may not be as effective as the others, but it does have a more acceptable side effect profile.
Surgical
When medical management is not effective, surgical techniques can be attempted.
These include:
- Trigeminal Nerve Branch Blockade, with the aim of providing anasethesia in the distribution of the nerve
- These can be attempted by neurectomy, alcohol injections or induction of radiofrequency lesions
- Unfortunately in some cases it results in ‘anaesthesia dolorosa’ which is intense pain in the area of sensory loss.
- Percutaneous damage to the Trigeminal Ganglion
- Radiofrequency thermocoagulation
- Glycerol injection causing chemical destruction
- Mechanical compression through balloon inflation
- Trigeminal root lesion caused by gamma knife
- Lesion just before it enters the pons.
- Microvascular decompression
- May be most efficacious intervention for classical trigeminal neuralgia
- There are complications
- Mortality is 0.3%
- CSF leak
- Brainstem infarctions
Reference
- Cruccu G et al. Trigeminal Neuralgia NEJM 2020;383:754-762







