
I’ve presented the ‘Imposters’ before, Here is a case of a STEMI that’s not a STEMI.
At a recent Cardiac Bootcamp I spoke about the 4 things I look for in an ECG to help me determine if there are signs of ischaemia on the ECG.
4 Things I look for to RULE IN ischaemia on an ECG
- If there is ST depression in any other lead except aVR and V1, it is ischaemia
- ST elevation III>II is a STEMI
- QR-T Sign or convex ST segment it is a STEMI
- Are there Hyperacute T waves (“T wave towards over the QRS in V3 or V4): It is a STEMI (check that it isn’t hyperkalaemia)
CASE 1(1)
A 57 yo male presents to the emergency department with central dull chest pain that started after going for a walk. There was no radiation but the patient had dyspnoea and fatigue. He had no past medical history and was on no medications.
He had a family history of his father having had a cerebrovascular event and mother a pulmonary embolism.
On examination he was afebrile, HR of 100bpm, BP of 102/60, respiratory rate of 22 and SaO2 of 95% on oxygen.
An ECG was done and is shown below:
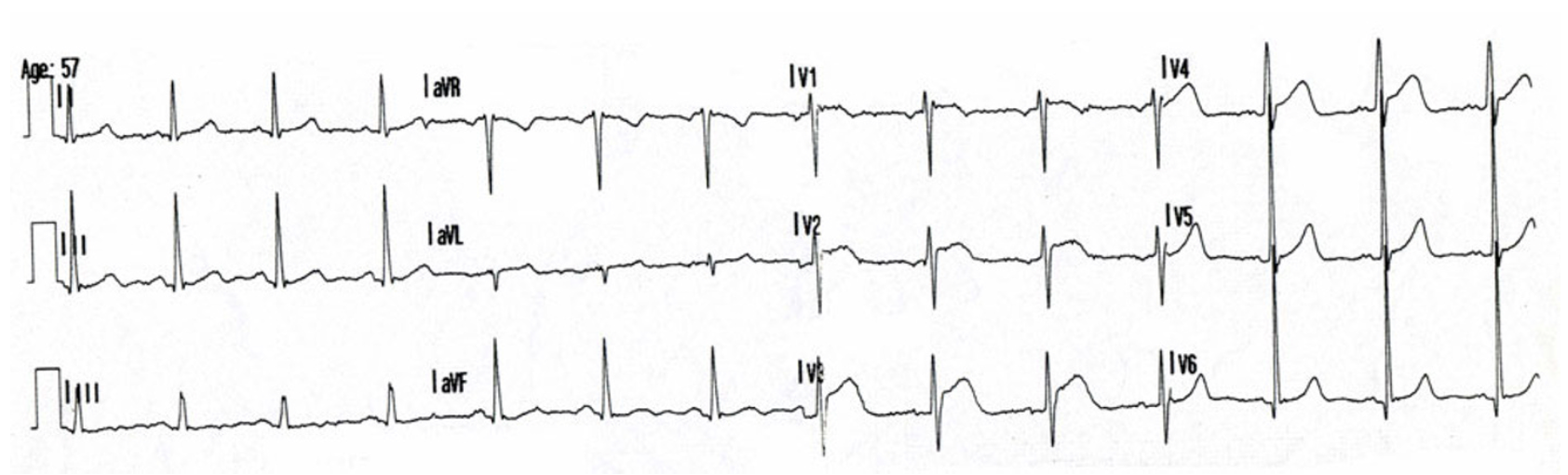
WHAT DOES THE ECG SHOW?
Sinus Rhythm
Incomplete RBBB
ST elevation V1-V4
What’s your diagnosis?
The assumption was an acute antero-septal myocardial infarction and the patient was taken to the cath lab.
Coronary angiogram showed: Normal coronaries. There was a small separate conus artery arising from the aortic root with embolic occlusion. However this was too small to stent. (The conus artery is usually the first branch of the right coronary artery, but in up to 50% can arise from a separate ostium from the right aortic sinus.)
An echocardiogram demonstrated normal left ventricular function, enlarged right cardiac chambers, with paradoxical movement of the interventricular septum and a right heart pressure of 40mm Hg and thrombi were seen in both pulmonary arteries confirming pulmonary embolism. He was then treated for this.
Ultrasound of the lower limbs showed a DVT.
The ST segments in the ECG normalised however the patient developed T wave inversion in the inferior leads.
WHY DOES THIS MIMIC OCCUR?
The cause is not really known although ST elevation in leads V1-V4 has been reported in the literature (2,3,4,5).
There are two theories:
- The right ventricle is very prone to ischaemia and doesn’t tolerate increased pressures very well. (read the Right Ventricular Spiral of Death). A pulmonary embolism results in sudden pressure increases in the right ventricle, that can result in both focal and global myocardia ischaemia. The ST elevation is due to epicardial or microvascular coronary vasospasm.
- A second theory relates to a catecholamine surge occurring with acute pulmonary embolism. This results in increased myocardial work resulting in ischaemia.
Conus artery embolism has been shown to cause ST elevation(6). Hence the possibility of paradoxical embolism must also be considered, especially if there is communication between the venous and arterial systems.
CASE 2 (7)
A 57 yo male presents to the emergency department following a syncopal episode at home. There was no prodrome. On awakening the patient had central chest pain and shortness of breath. The patient had a significant coronary artery disease history with previous cardiac stents. Past medical history also included hypertension, hyperlipidaemia and renal impairment.
He was afebrile, HR of 111bpm, BP 123/80 SaO2 96%
The initial ECG is shown below:
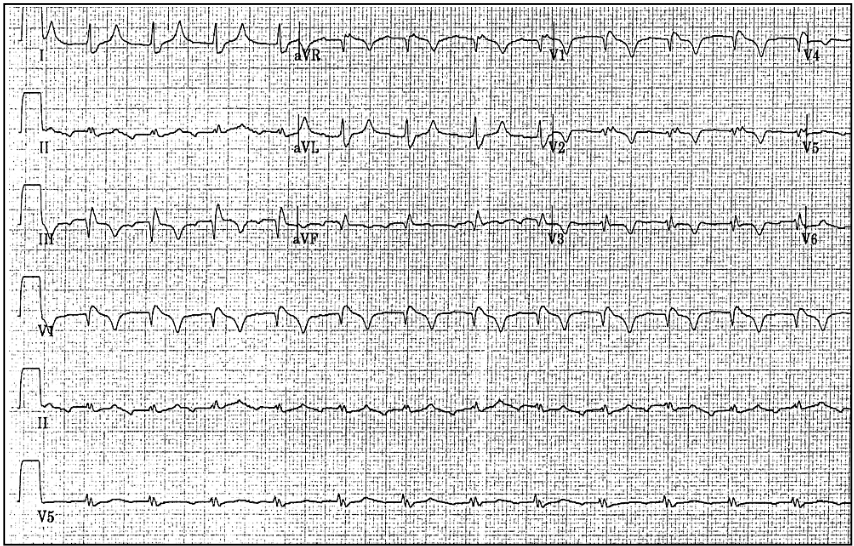
WHAT DOES THE ECG SHOW?
Sinus rhythm
Incomplete RBBB
Anterior and inferior T wave inversions.
Q waves in the inferior leads.
A second ECG was done some time later and showed the following:
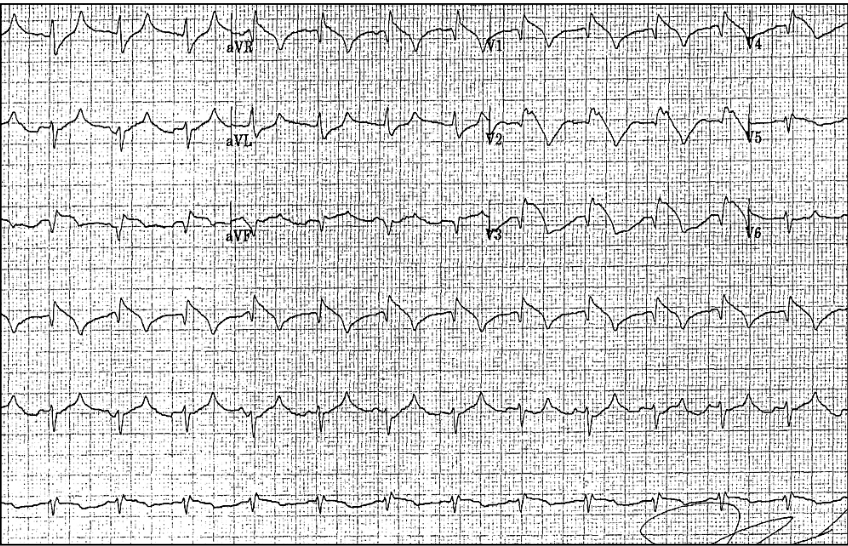
WHAT DOES THE ECG SHOW?
ST elevation in the anterior and inferior leads.
What is your diagnosis now?
The patient was given GTN, following which the blood pressure dropped and the GTN was removed. Was this a clue that this could be right heart related?
An acute occlusion was suspected and the patient was taken to the cath lab.
Cardiac catheterisation demonstrated patent stents and no occlusive lesions.
Transthoracic echocardiography revealed right ventricular enlargement and displacement of the interventricular septum, with elevated right sided pressures and normal left ventricular function. Pulmonary embolism was suspected and a V/Q scan showed large bilateral ventilation-perfusion mismatches. The patient was treated for pulmonary embiolism.
CONCLUSION
We need to consider the diagnosis of acute pulmonary embolism in patients with ST elevation in the praecordial leads, especially if the history has elements relating to dyspnoea.
REFERENCES
- Goslar T et al. Acute ECG ST-segment elevation mimicking myocardial infarction in a patient with pulmonary embolism. Cardiovascular ultrasound. 2010 :50
- Falterman TJ, et al: Pulmonary embolism with ST segment elevation in leads V1 to V4: case report and review of the literature regarding electrocardiographic changes in acute pulmonary embolism. J Emerg Med 2001, 21(3):255-61.
- Wilson GT, Schaller FA: Pulmonary embolism mimicking anteroseptal acute myocardial infarction. J Am Osteopath Assoc 2008, 108(7):344-9.
- Lin JF, Li YC, Yang PL: A case of massive pulmonary embolism with ST elevation in leads V1-4. Circ J 2009, 73(6):1157-9.
- Livaditis IG, et al: Massive pulmonary embolism with ST elevation in leads V1-V3 and successful thrombolysis with tenecteplase. Heart 2004,90(7):e41
- Kagiyama S, et al Transient precordial ST elevation by a spasm of the conus artery during right coronary angiography. Int J Cardiol 2007, 116(2):e57-9






Case 2 has S1Q3T3. While this has terrible sensitivity/specificity, in context of syncope, I’d think PE should be #1 suspicion.