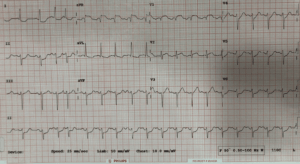
A 70 year old woman presents with severe shortness of breath and chest pain. She loses output briefly. Her ECG is shown below She has ST elevation in aVR. What is the diagnosis? Read below and then view the angiogram.
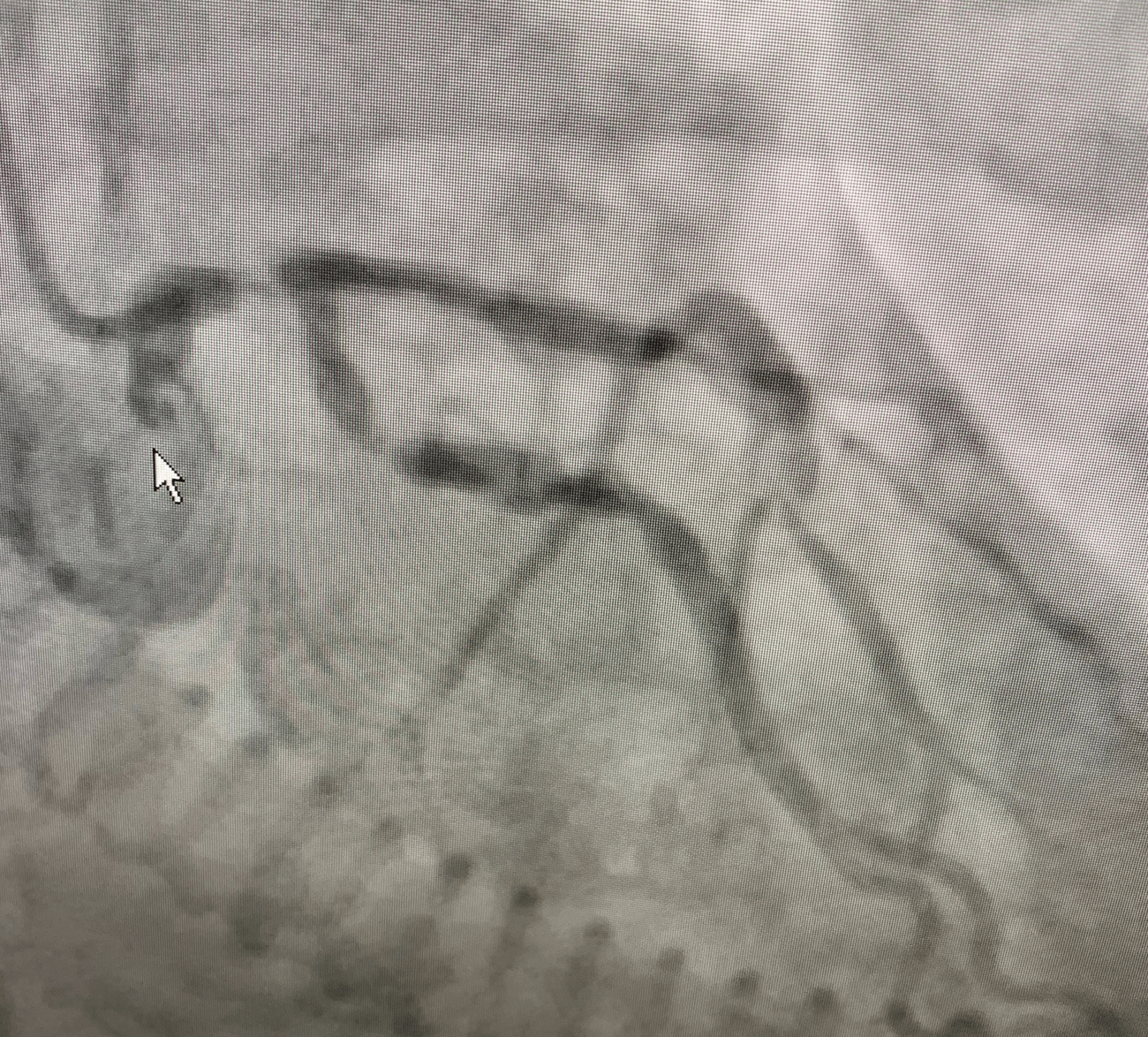
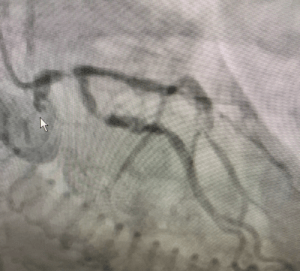
We diagnosed critical Left Main Coronary Artery(LMCA) obstruction and urgently transferred the patient for angiography and potential coronary artery bypass graft(CABG).
Anatomy and lead aVR
aVR looks at the right upper heart, giving us a reciprocal view of I, II aVL and V4-6. Thus ST elevation in aVR is usually associated with an obstruction of the proximal Left Anterior Descending(LAD) artery(1). LMCA occlusion is associated with posterior wall ischaemia, therefore producing reciprocal changes in the precordial leads.
ST elevation in aVR may indicate:
- Critical LMCA occlusion. Remember that it will usually not be total occlusion, as this will lead to rapid cardiac arrest and death. Think of this in the presence of ST elevation in aVR and ST depression in I, II, aVL and V4-6.
- Triple vessel disease
- Proximal Left Anterior Descending (LAD) artery occlusion; usually proximal to the major septal branch, when it occurs in the presence of anterior ST elevation
- It can be benign as in Supraventricular tachycardia (SVT)
Things to consider
The degree of elevation of the ST segment in aVR correlates with mortality and its relationship to the ST elevation in V1 can give clues as to the location of the lesion.
ST elevation in aVR of > 1mm in the presence of non-ST elevation in the precordial leads has a sensitivity of 80% and a specificity of 93% for LMCA or triple vessel disease(2)
When the ST elevation in aVR > V1, it is more likely to be a LMCA rather than LAD occlusion(3).
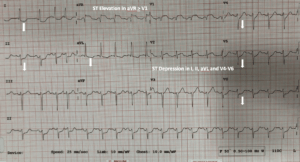
Let’s look at the ECG again. There is ST elevation of aVR > V1 and ST depression of I, II aVL and V4-6. The prediction is a critical LMCA occlusion. The angiogram below showed a critical LMCA occlusion into the bifurcation. In these patients discuss with cardiology before giving Clopidogrel, as they may need to have CABG and the drug is associated with increased bleeding in these cases.
References
- Engelen DJ et al. Value of electrocardiogram in localising the occlusion site in the left anterior descending coronary artery in acute anterior myocardial infarction. J Am Coll Cardiol 1999;34:389-395
- Kosuge M et al. An early and simple predictor of severe left main and/or three vessel disease in patients with non-ST-elevation acute coronary syndrome. Am J Cardiol Feb 15 2011Vol 107, issue 4:495-500(abstract)
- Yamaji H et al. Prediction of acute left main coronary artery obstruction by 12 lead electrocardiography: ST segment elevation in lead aVR with less ST segment elevation in lead V1. J Am Coll Cardiol November 2001. Vol 38, Issue 5: pp1348-1354







