
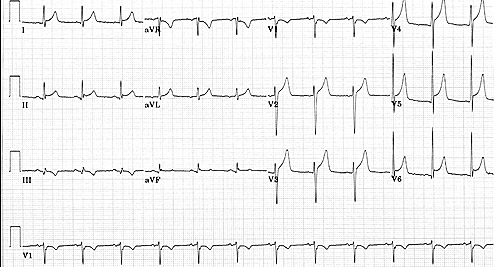
A 28 year old male presents with atypical chest pain, shortness of breath and a feeling of general muscular aches and pains. He has an ECG. Does it show early repolarisation or an infarction, or something else?
In this ECG, there is ST elevation in the inferior and anterior leads. What do you think?
What are the causes of ST Elevation?
- Acute AMI
- Benign Early Repolarisation
- Pericarditis
- Left ventricular Aneurysm
- Bundle Branch Block
How to distinguish Benign Early Repolarisation from AMI, or even pericarditis?
The things I look for in the ECG to diagnose early repolarisation are:
- ST elevation of <2mm
- The morphology of the ST segment ie a concave segment
- A notch or slurring of the terminal QRD complex
- That there are no reciprocal changes
- ST elevation is diffuse ie., not in an arterial territory
- There is a concordant T wave of large amplitude
- There are no dynamic changes

When I look at an ECG the first 4 predictors of early repolarisation are of greatest importance ie.
- ST elevation <2mm
- Concave segment
- Notching of terminal QRS complex
- No reciprocal changes
ALWAYS look at the ECG with the history in mind. In an older patient with a good history, I would treat as for myocardial ischaemia.
If the patient gives a great history of AMI, then I re-look at it, test it for dynamic changes and get another opinion.
Why is this all so important? Primarily it’s about the right management and about risk management. No-one wants to thrombolyse benign early repolarisation, or pericarditis; the potential complications are devastating, or are they? In 2016 I spoke on this at the Cardiac Bootcamp. It is not that uncommon for thrombolytics to be given for pericarditis mistaken as an infarction. How there is under-reporting.
Here’s another ECG, of a 30 year old male with atypical chest pain and generalised muscular aches and pains:
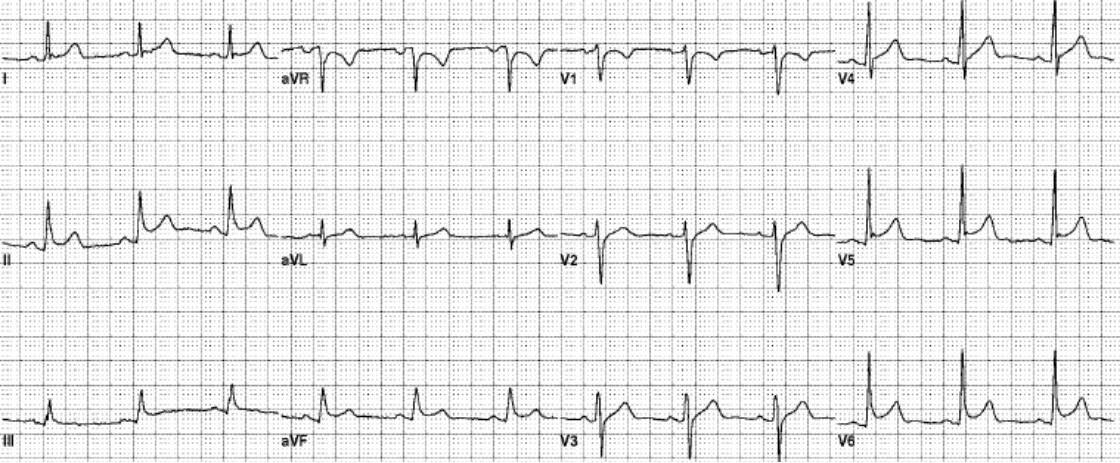
Again the ECG shows changes in both the inferior and anterior leads, i.e.., not restricted to arterial supply and not reciprocal.
Can we differentiate this from pericarditis and how? That’s the next blog.
EARLY REPOLARISATION MAY NOT BE AS BENIGN AS YOU THINK? Keep tuned for an update.








Peter and Chance you could explain reciprical changes on ECG regards
Mark Loeffler
Hi Mark
A reciprocal change is simply an ST depression in leads other than those where there is ST elevation. That means that to have reciprocal changes you must have ST elevation. Reciprocal changes or ST depression in the presence of ST elevation assists in the confirmation that the ST elevation is in fact ischaemic. It also identifies a subgroup of patients at risk of cardiovascular complications.
Peter