THE CASE
A 35yo patient presents with multiple complaints which include:
- lower abdominal pain
- retrosternal chest pain
- lumber back pain and
- numbness and weakness in both legs
This is a previously well patient with no significant medical history. This morning, the patient noticed some mild flu-like symptoms on waking. During the day the patient felt severe cramping abdominal pain that was burning in nature. It radiated to the epigastrium and retrosternally.
The patient then developed burning pain between the scapulae as well as lumbar back pain. This was followed by numbness and weakness of both legs, with the numbness extending to the abdomen.
The patient was unable to stand and pass urine.
On general examination, the patient was alert and in no distress. The vitals were normal, there were dual heart sounds with no extra sounds, a clear chest and a soft abdomen with a mild epigastric discomfort.
Spinal examination demonstrated some tenderness over L5. The neurological examination demonstrated sensory loss from T10 distally to fine touch and pain. The lower limbs had normal tone bilaterally. Power was 0/5 in the right leg, but better on the left with 3/5 power at the ankle and knee and 1/5 at the hip. Both plantars were down-going and no reflexes could be illicited.
DIFFERENTIAL DIAGNOSIS
The main differentials to consider are:
- Haematomyelia (intraspiral haemorrhage)
- Myelopathy
- Transverse myelitis
- Demyelinating Disease
- Acute Disseminated Eucephalomyelitis
- Dissection
- Neurosyphilis
- Tumour
- VaricellaVasculitis
Investigations
Bedside – BSL
Labs – FBC, ESR, Electrolytes, Syphilis serology.
- Leulocytosis may indicate infection
- Hypokalaemia may result in weakness.
Let’s look at some of the differentials in more detail
BROWN-SEQUARD SYNDROME
It results from damage to one half of the spinal cord.
The clinical findings are:
On the side of the injury
-
Paralysis (loss of motor function)
-
Loss of proprioception
On the Contralateral side
-
Loss of pain
-
Loss of temperature
It is usually caused by trauma (such as gunshot wound or other puncture wound (see blog), by a spinal cord tumour, ischaemia, infection or inflammation (multiple sclerosis, tuberculosis).
This is a rare condition, with no treatment.
For a trauma case of Brown-Sequard click here.
TRANSVERSE MYELITIS
This occurs due to an inflammation of the nerve fibres of the spinal cord resulting in a loss of myelin coating and a reduction in electrical conductivity. It can be total or it can be partial.
AETIOLOGY
Infectious
-
Bacterial: Mycoplasma Pneumonia, Lyme Disease
-
Viral: Herpes infections, EBV
Multiple Sclerosis
Paraneoplastic Syndromes
Vascular
PRESENTATION
It can occur in all levels of the spine. The thoracic cord is the most common and results in a weakness of lower limbs.
It also occurs in upper motor neurone signs in the lower limbs, the patient having spastic diple
If the lesion occurs in the lumber region of the spinal cord (L1-S5), there may be a combination of upper and lower motor neuron signs.
Cervical cord involvement may result in quadriplegia, or a combination of upper and lower motor neuron signs if the lesion is low cervical.
A mid cervical lesion can result in respiration paralysis.
SPINAL CORD INFARCTION
Presentation
Spinal cord infarction has an acute onset. In more than 80% of cases, it starts with severe spinal back pain.
It is most commonly thoracic and presents with partial or complete paralysis of the lower limbs, sensory loss and inhibility to void.
In the first few days, spinal shock occurs, where the limbs have a lack of tone, are flaccid and are flexic.
In most cases, the lesion is located in the anterior 2.3 of the chord, sparing posterior columns and thus vibration and position sense.
Light touch is also preserved, however pain and temperature sensation are lost.
Aetiology
The following are some of the causes:
-
Arteritis
-
Dissecting aneurysms
-
Trauma
-
Emboli
-
Decompression illness
BEWARE FALSE LOCALIZING SIGNS
Although a rare phenomenon, patients with a sensory thoracic level may in fact
have a cervical lesion from 6-11 segments away. (Clin Neurol Neurosurg 2013, Jan j115 (1) 546).
In patients with a thoracic level and a normal MRI at this level should be further evaluated with cervical spinal cord and brain imaging.
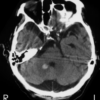
MRI RESULTS of the patient in this case
The patient in this case had an MRI which demonstrated increased T2 signal, with owls eye appearance.
There was mildly increased STIR sign at T3-4 although this does not demonstrated restricted diffusion.
The differentials given were transverse myelitis or spinal cord infarction.
The Diagnosis was spinal cord infarction.