
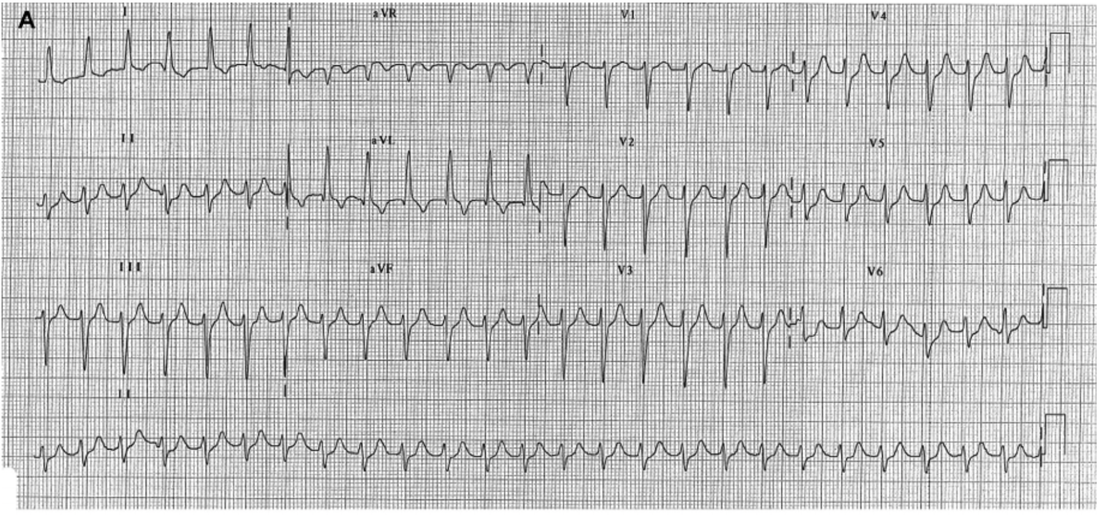
A 79 yo male presents with palpitations. He is haemodynamically stable with a BP of 138/68. His ECG is shown below. What does it show?
Ann Noninvasive Electrocardiol 2015;20(4):314–327
ECG: A narrow complex regular tachycardia with a ventricular rate of 145, but no visible P waves.
You think it’s some type of SVT, so you try vagal manoeuvres including the new REVERSE Vagal Manoeuvre. However there is no response.
You decide to give Adenosine.
Your colleague asks “Are you sure you want to give adenosine?”
Your response is: “It’s a regular narrow complex, so Adenosine should be fine. If it were irregular ie., atrial Fibrillation and there were wide complexes indicating it might be atrial fibrillation with WPW, then I wouldn’t give it. We should be OK”. (members go to ECG’s, when giving the wrong drug can kill your patient)
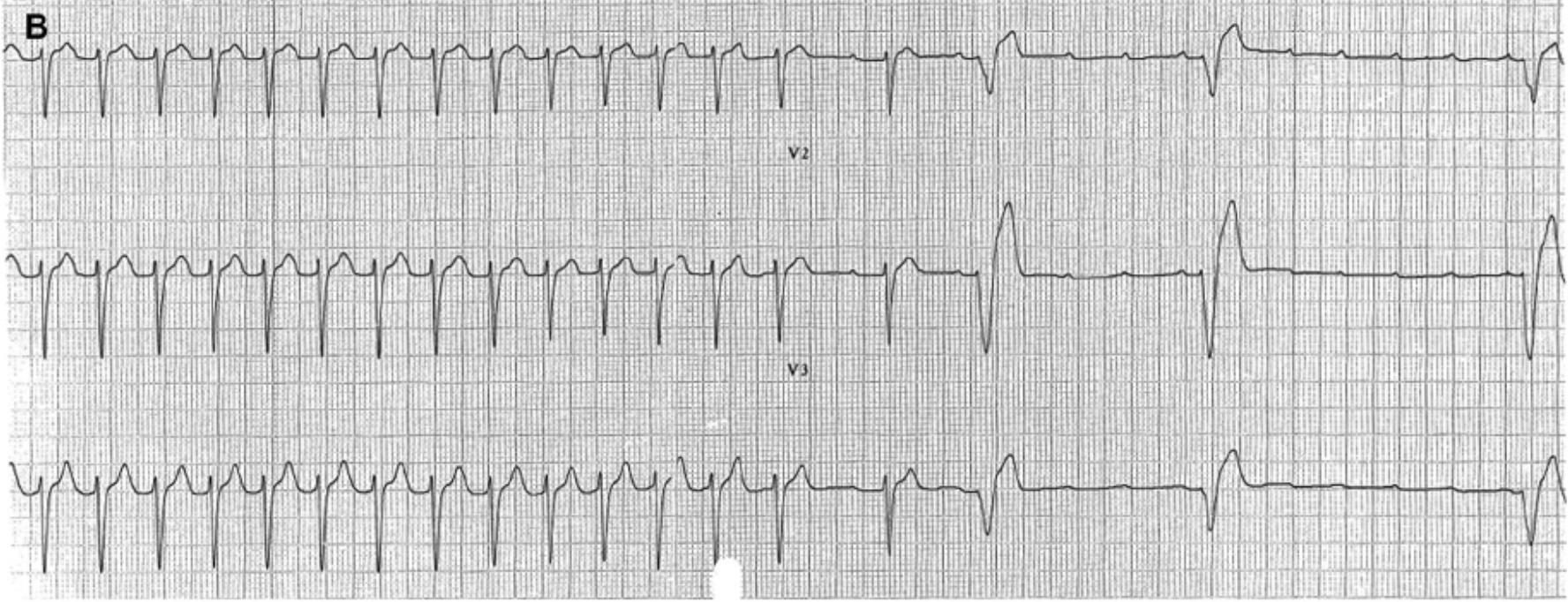
You give Adenosine and the following ECG is taken. What does it uncover?
You think it’s some type of SVT, so you try vagal manoeuvres including the new REVERSE Vagal Manoeuvre. However there is no response.
You decide to give Adenosine.
Your colleague asks “Are you sure you want to give adenosine?”
Your response is: “It’s a regular narrow complex, so Adenosine should be fine. If it were irregular ie., atrial Fibrillation and there were wide complexes indicating it might be atrial fibrillation with WPW, then I wouldn’t give it. We should be OK”. (members go to ECG’s, when giving the wrong drug can kill your patient)
You give Adenosine and the following ECG is taken. What does it uncover?
Ann Noninvasive Electrocardiol 2015;20(4):314–327
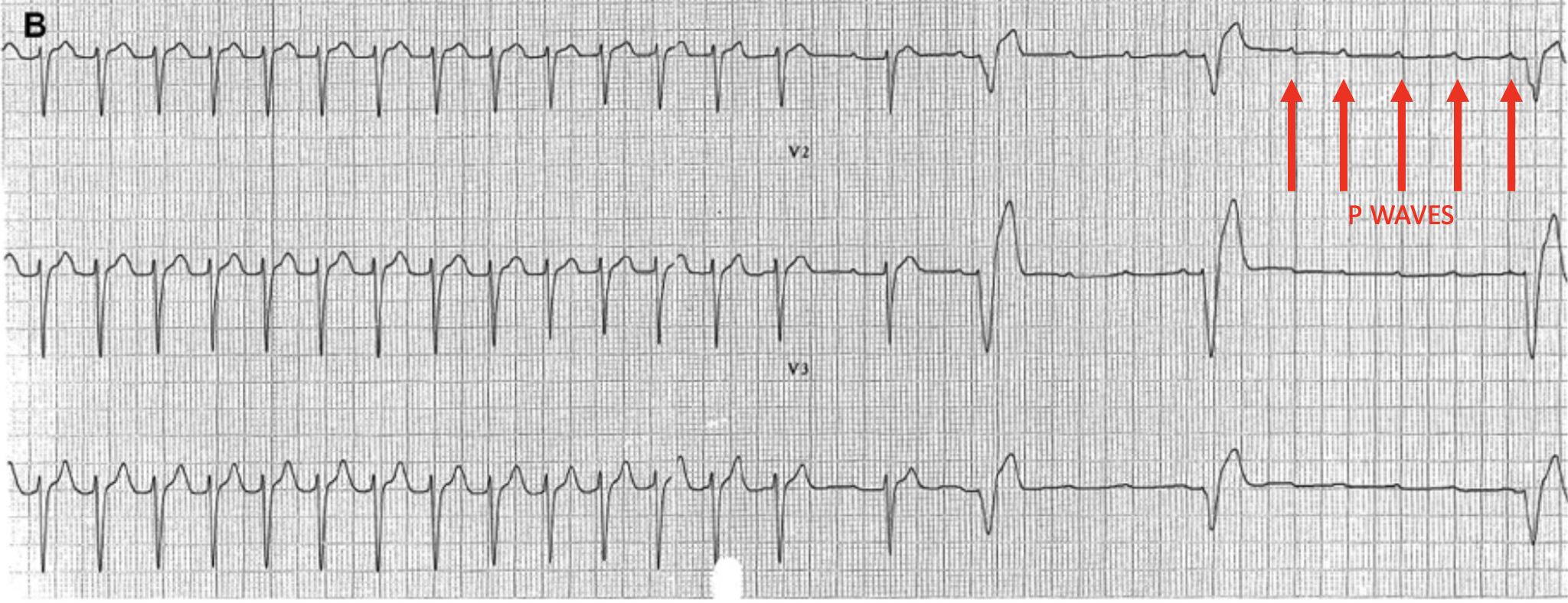
As the ventricular beats are blocked, the p waves become evident and the underlying atrial tachycardia is uncovered. We can sometimes use the LEWIS LEAD to make p waves more prominent, however the rate may make that difficult to do here.
Atrial Tachycardia
It is a type of supraventricular tachycardia that can occur in both normal hearts and in congenital heart disease.
The ECG usually has the following characteristics:
- Rate > 100bpm
- If seen the P waves have an atypical morphology
- There is a narrow QRS
We think of Atrial tachycardias as falling into 3 groups:
- Focal Atrial Tachycardia
- It is REGULAR
- Localised to one atrial focus
- There are discrete P waves
- Usually caused by catecholamines/stimulants, digoxin and alcohol.
- Multifocal Atrial Tachycardia(MAT)
- It is IRREGULAR because because of multiple foci firing at different times
- There are 3 different P wave morphologies
- Re-Entrant Atrial Tachycardia
- Usually persistent
- Occur after cardiac surgery or ablation
MANAGEMENT
- These atrial tachycardias are usually self terminating and except for some cases of congenital heart disease are usually not life threatening.
- Focal atrial tachycardias may respond to cardioversion, however MAT DOES NOT.
- Class Ia and Ic anti-arrhythmics such as Flecainide, have some effectiveness, however we have to be sure that there are no structural abnormalities (ie., ECHO is needed) as they can be arrhythmogenic.
- Class III drugs such as Amiodarone and Sotalol, although not effective in terminating the arrhythmia are good for maintaining a sinus rhythm.
- If the patient has a re-entry atrial tachycardia, AV nodal blockers are unlikely to terminate, however cardioversion is appropriate in unstable patients.
OTHER INVESTIGATIONS
What other investigations may be appropriate?
LABS
- Electrolytes,
- Haemoglobin,
- Digoxin levels
RADIOLOGY
- CXR, looking for COPD,
- CTPA if suspicious for a PE
- ECHOCARDIOGRAPHY to look for structural heart disease, left atrial size and pulmonary arterial pressure.







