His vitals are:
HR 170 beats per minute in a narrow complex tachycardia
BP 110/60
Sats 96% on RA
T 36.1
He is placed in an acute cubicle and monitoring is attached.
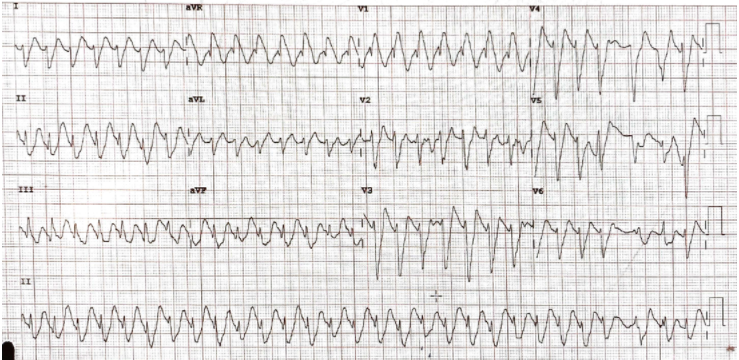
As an ECG is being done, the nurse calls for a doctor urgently ‘He’s gone into a wide complex tachycardia!” The ECG is shown below:
What is the rhythm?
(a) Ventricular Tachycardia
(b) SVT with RBBB
(c) Hyperkalaemia
(d) Na channel Blockade
(e) Acute Myocardial Infarction
What favours Ventricular Tachycardia?
What favours SVT + RBBB?
How would you treat this patient?
When should Amiodarone not be given in an ECG like this?
He was shocked twice, with no resolution.
Why was this and what would you do next?
This is a great ECG.
Let’s systematically go through it and apply the ‘120 CRAM‘ formula
Firstly we’ll remind ourselves of the causes of wide complex tachycardia:
Remember these causes:
- Ventricular Tachycardia
- SVT with Aberrancy
- Hyperkalaemia
- Na+ Channel Blockade
- Ischaemia
- Paced Rhythm
I like going over all of these in my head, for every patient with a wide complex tachycardia.
Let’s work through it:
120: Is it faster than 120bpm and wider than 120ms but no too wide?
It’s faster than 120bpm and wider- perhaps too wide. If the complexes are > 1 large square think hyperK.
In this case the K was 6.7mmol/L. We could stop there and treat with Calcium and add some bicarb and we could be done. But let’s dig a little deeper and look at what else points to and against VT.
Beware giving the patient with hyperkalaemia Amiodarone as the K channels are already poisoned and the Amiodarone will poison the Na+ channels, which can result in asystole.
C: Concordance
There is no concordance in the anterior leads, so this is against VT
R: R wave in aVR
There is no initial dominant R wave in avR, it’s an RSR, so this is against VT
However if we look at aVR, there appears to be a terminal R wave consistent with Na channel blockade.
Does this look like a RBBB?
If we look at lead V1 , it has an rsR morphology, very similar to a RBBB. If it was VT it would have an Rsr morphology(remember the rabbit’s ear). Plus we see that there is a rightward axis.
So so far it is looking like a hyperK + Na channel blockade + RBBB
A: AV dissociation
I can see p waves in V2. Is it dissociated? Hard to see that. Can you? It may be that the initial upstrokes in aVR are p waves.
Morphology
Are there fusion or capture beats?
There may be some towards the end of the ECG, in the last few complexes, but I’m not sure.
Given that there is right bundle branch block morphology we look for 3 things:
- Right Rabbit Ear(V1)- Not present
- There is no pure R wave in V1, however the RS interval is > 100ms
- qR(v1)- Not present
- R/S < 1 in V6- Present
So there are a few features here that might indicate VT.
CONCLUSION
I have presented this case in this way to you, to illustrate that applying the 120CRAM or any other algorithm can be confusing no matter how many you’ve done it before.
The following are important in this case:
- Can amphetamine toxicity cause Na channel blockade-like ECG appearance?
- We have hyperK here, so why consider VT?
- There are some parts that fit into VT and some that don’t.
My view is that this is not VT but is a combination of the high K and the amphetamine overdose and a RBBB.
What are the ECG effects of amphetamines?
Amphetamine overdose can result in significant ECG changes which include:
- Sinus tachycardia
- Prolonged QT interval
- Tall T-waves
- ST segment elevation
- Anterior myocardial infarctions
- Arrhythmias which included:
- ventricular tachycardia,
- premature atrial contractions,
- paroxysmal supraventricular tachycardia and
- premature ventricular contractions.
So to confuse matters further, we see that amphetamines can cause ventricular tachycardia.
The patient had cardioversion attempted twice, with no effect, probably because this was not VT. The patient received calcium and bicarbonate.
The complexes narrowed.
So this was a Hyperkalaemic ECG with some Na channel blockade characteristics.
What would have happened if the patient had received Calcium early? It may have narrowed the complexes early.
A difficult case, but one that reinforces the approach we teach at Cardiac Bootcamp.
< strong style=”color:rgb(102, 102, 102)”>The Approach:
If at any time the patient is unstable, cardioversion is the option. If it isn’t VT, nothing will happen
- It will be VT in > 80% of cases as long as it is regular, and faster than 120bpm and wider than 120ms. If unstable shock’em. If stable you have time to think.
- If it’s too wide, (usually > 1 large square), think hyperkalaemia and test the Potassium. In fact, if the patient is haemodynamically stable, check the potassium on every one of these patients with a wide complex tachycardia anyway.
- Consider giving Calcium here.
- Is there a time not to give Calcium? You will have read to not give Calcium in the presence of hyperkalaemia in digoxin toxicity. The concern being ‘stone heart’, although there is not much evidence of this.
- If you believe it is an SVT with a bundle branch block, you can give adenosine, but only if it’s regular (not if fast atrial fibrillation) as we don’t want to give an AV nodal blocker to a patient with AF with WPW, as the patient will develop ventricular fibrillation(read the section on drugs that can kill your patient)
- If you give Adenosine and it’s SVT, it will ‘break’ the arrhythmia
- If it’s VT, it will do nothing as VT originates in the ventricle(there is one exception, but we won’t worry about that for now).
- If the K+ is normal and you are happy it’s not Na+ channel blockade and it doesn’t revert with Adenosine, and you are happy it’s not one of the other causes, then you can try and revert with Amiodarone
- Remember, if in doubt shock.
Let me know what you think







