
A 31 yo female presents to the emergency department with pleuritic chest pain. The patient is 19/40 gestation and no medical conditions. The history of the event is that the patient was sitting on the couch and developed left shoulder and then left chest pleuritic chest pain. There was no history of trauma, or fevers, cough or wheeze and the patient had no history of a DVT.
Clinical examination was normal.
Basic blood tests were done that showed:
CRP 4
D-Dimer 0.71 mg/L
Na 134/ K 4.1/ HCO3 19/ Creat 61/ eGFR 90
WCC 10.4/ Neut 6.3/
High sensitivity troponin 3
Vitals were HR 80bpm, BP 122/70 SpO2 100% on RA.
What is your working diagnosis so far?
An ECG was done as shown below. The resident reported it as normal. What does it show and what is your diagnosis?
Clinical examination was normal.
Basic blood tests were done that showed:
CRP 4
D-Dimer 0.71 mg/L
Na 134/ K 4.1/ HCO3 19/ Creat 61/ eGFR 90
WCC 10.4/ Neut 6.3/
High sensitivity troponin 3
Vitals were HR 80bpm, BP 122/70 SpO2 100% on RA.
What is your working diagnosis so far?
An ECG was done as shown below. The resident reported it as normal. What does it show and what is your diagnosis?
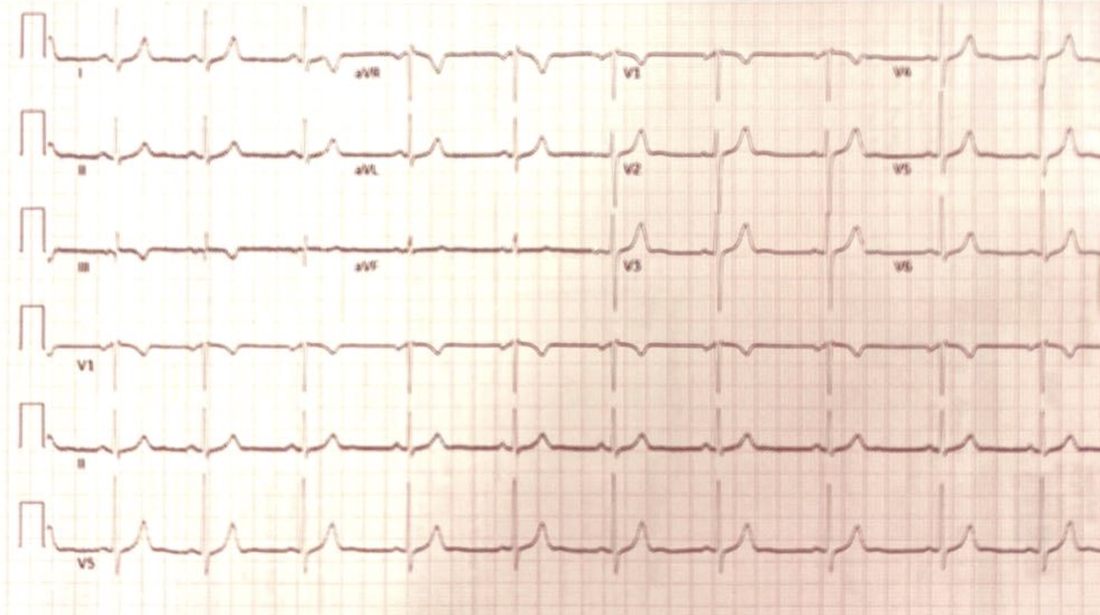
ANSWER
This is a normal sinus rhythm ECG, with good R wave progression. The only finding of note is S1Q3T3
What are some of the important ECG changes seen in Pulmonary Embolism?
- S1Q3T3- +ve LR 3.7 of a PE(1), although often said to be neither sensitive nor specific.
- RBBB
- T wave inversion V1-V4 +ve LR 3.7
- Tachycardia +ve LR 1.8
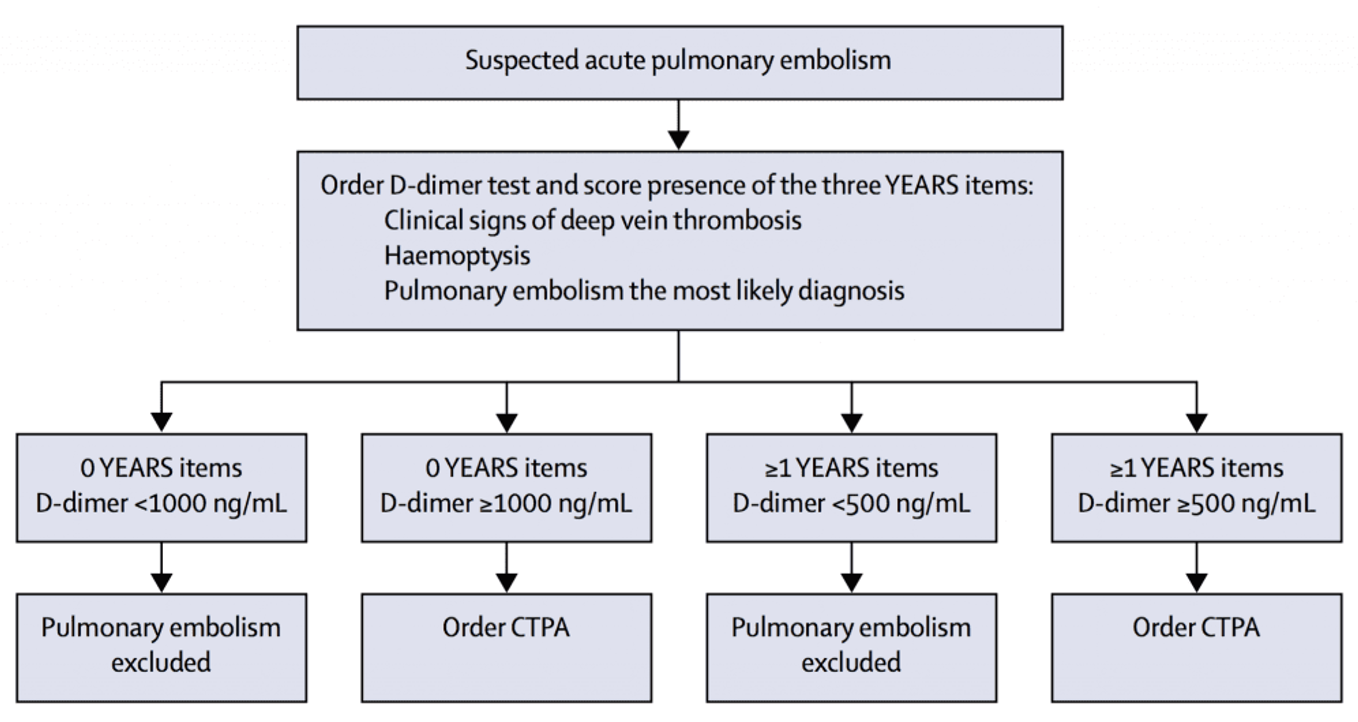
What did the YEARS Study tell us?
In 2017, we were given a new approach to looking at PE and the D-dimer(2)
They used a clinical decision rule which consisted of 3 items:
- Clinical Signs of Deep Venous Thrombosis
- Haemoptysis
- Is Pulmonary Embolism the Most Likely Diagnsosis?
The flow diagram is shown below, but in summary it says:
In the non-pregnant patient:
- If no criteria can rule out PE with d-dimer of <1000 ng/mL
- If criteria can rule out PE with a D-dimer of <500ng/mL
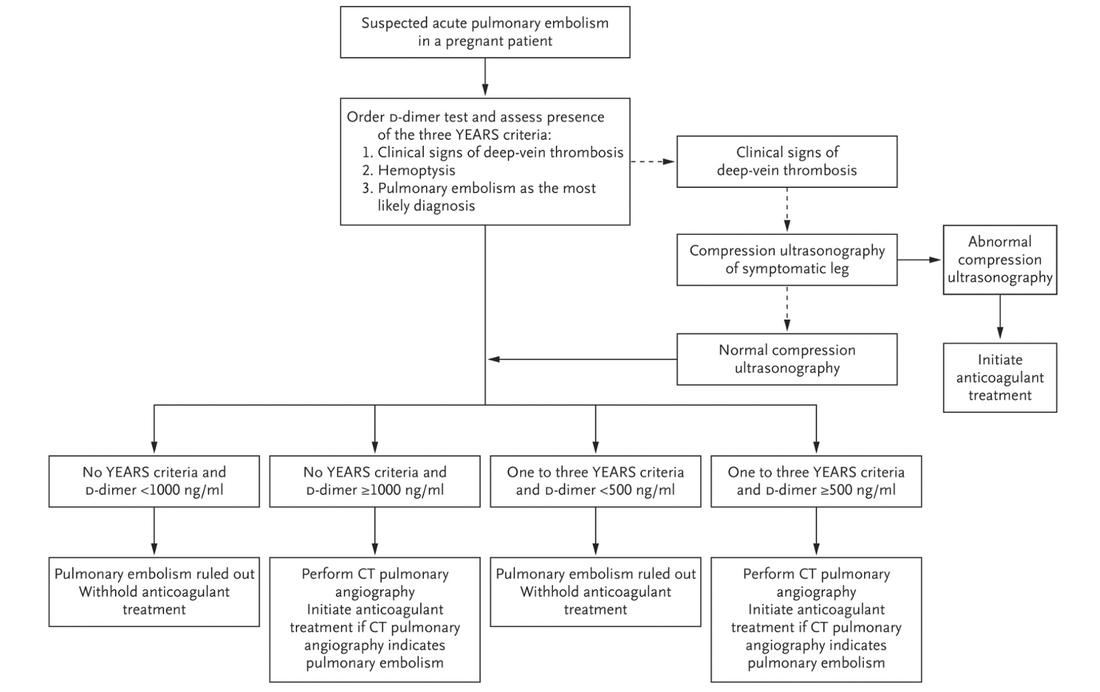
In the pregnant patient:
- If no criteria can rule out PE if D-dimer is < 1000 ng/mL
- If criteria can rule out PE if D-dimer is <500 ng/mL
OVERALL
- In any patient with NO CRITERIA a D-dimer of <1000 ruled out PE
- In any patient WITH CRITERIA a D-dimer of < 500 rule out PE
The Pregnancy Adapted algorithm from 2019(3) is shown below:
WHAT HAPPENED TO THE PATIENT?
It was decided that although pleuritic chest pain was all that the patient had, there was nothing else to explain the symptom. The D-dimer was > 500, so the patient was sent for a CTPA. It was negative. The patient was discharged for GP followup.
Members, go to the section on PE in the course and on the ECG’s of PE to see more.
References
- Marchick M.R. et al. 12 Lead ECG Findings of Pulmonary Hypertension occur more frequently in Emergency Department patients with Pulmonary Embolism than in patients without Pulmonary Embolism. Annals of Emergency Medicine. Vol 55, Issue 4, April 01, 2010; pp 331-335
- Van der Hulle T et al. Simplified diagnostic management of suspected pulmonary embolism (the YEARS study): a prospective, multicentre, cohort study. Lancet. 2017; 390:289-297.
- Van der Pol L.M et al. Pregnancy-Adapted YEARS Algorithm for Diagnosis of Suspected Pulmonary Embolism.N Engl J Med 2019; 380:1139-1149







