The right ventricular spiral of death in PE is very real and very scary. We sometimes miss it, because we treat all resuscitations the same way and we shouldn’t.
Here are two cases:
CASE 1: A 35 yo woman presents to the ED with SOB, tachycardia, BP of 105/60, a high respiratory rate and sats of 94% on room air. You are suspicious for a pulmonary embolism(PE) and get a CTPA, which confirms a large PE. Whilst in the resuscitation cubicle the patient’s blood pressure drops to 74/40
CASE 2: A 58 yo male presents with chest pain. He has a past history of hypertension and hypercholesterolaemia. The patient’s vitals are: HR 48 bpm, BP 110/60 sats 95% on room air. An ECG is done that reveals an inferior infarct. Right Ventricular leads show a Right Ventricular infarction. Whilst in the resuscitation cubicle the patient’s blood pressure drops to 74/40.
Do we treat these patients in the same way to stabilise the blood pressure? Certainly definitive treatment for each of the conditions, should treat the BP, but what do we do in the interim?
We tend to give 1-2 Litres of fluid. Should we be treating a right ventricular infarct, the same way as we treat a pulmonary embolism? Should we treat it in the same way as we treat sepsis, or even a Left ventricular infarction?
The answer is NO. At EMCORE, I will speak on “My Obsession with The Right Ventricle”. Here is a small part of that talk: what usually happens in PE………The Right Ventricular Spiral of Death……..
Differences between the Right and Left Ventricles
- The LEFT Ventricle is perfused in Diastole
- The RIGHT Ventricle is perfused in Diastole AND Systole ie., the whole cycle.
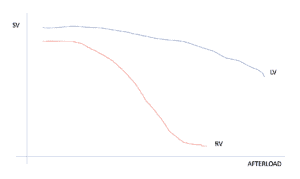
- The Right Ventricle doesn’t handle resistance(after load) very well.
Let’s Talk about PE
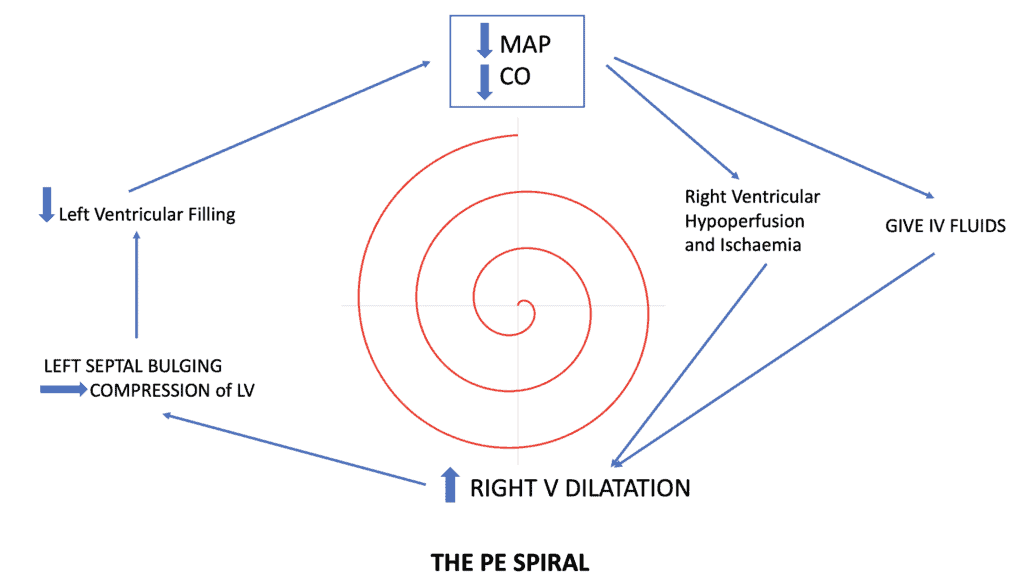
Our first response to the haemodynamically unstable patient is to give fluid. We can give one litre, maybe two. It doesn’t matter which fluid we give, the results are the same. Why do we give it? We believes it helps….. In the case of PE it harms, unless the patient is hypovolaemic.
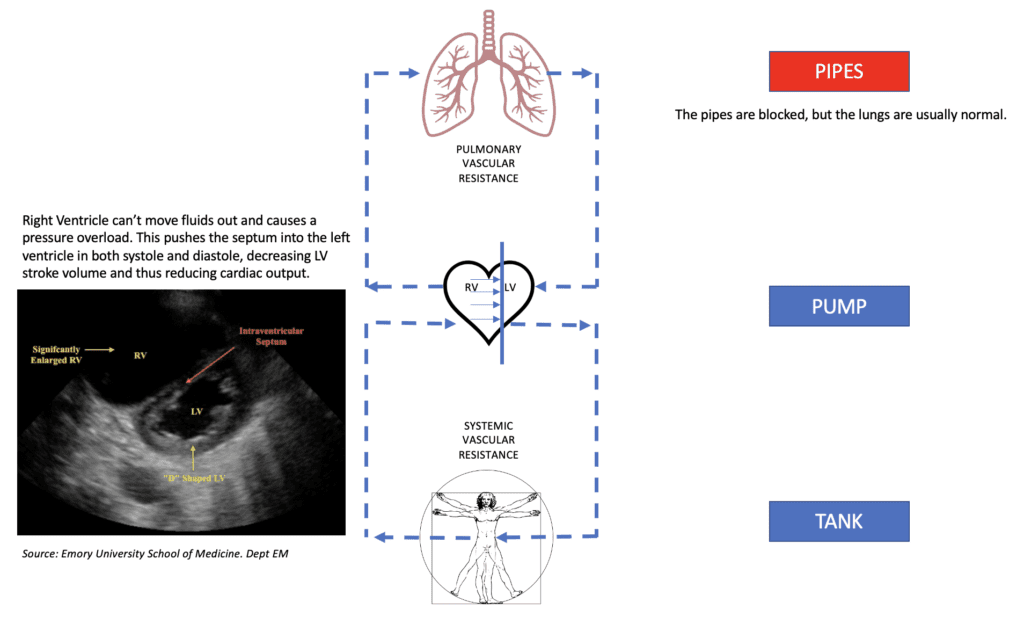
The increased fluid given can’t be pumped forward as there is a blockage in the ‘pipes’ ie., the pulmonary vasculature. With increased fluid and poor Right ventricular contractility, now due to ischaemia, there is an increase in Right ventricular volume, which leads to septal shift, increasing left end diastolic pressure and decreasing left ventricular preload, which decreased cardiac output. The further the drop in blood pressure, the more fluid we give……and so the right ventricular spiral of death continues.
If we use the old analogy of the Pipes/Tank/Pump model, then in PE the issue is a blockage in the pipes. The lungs are usually normal. If we do an ABG, we will usually find that the paCO2 > EtCO2, that is because CO2 is not entering the lungs to be cleared (see this gas example), due to a pipe blockage(vascular blockage). Apart from a mechanical blockage due to clot, there is also an inflammatory response and resultant pulmonary hypertension. See the figure below for an explanation.
The Pump, Pipes, Tank Model
If we look at this simplified model of what happens to the heart and lungs and the body.
Pump/Pipes/Tank: Pulmonary Embolism
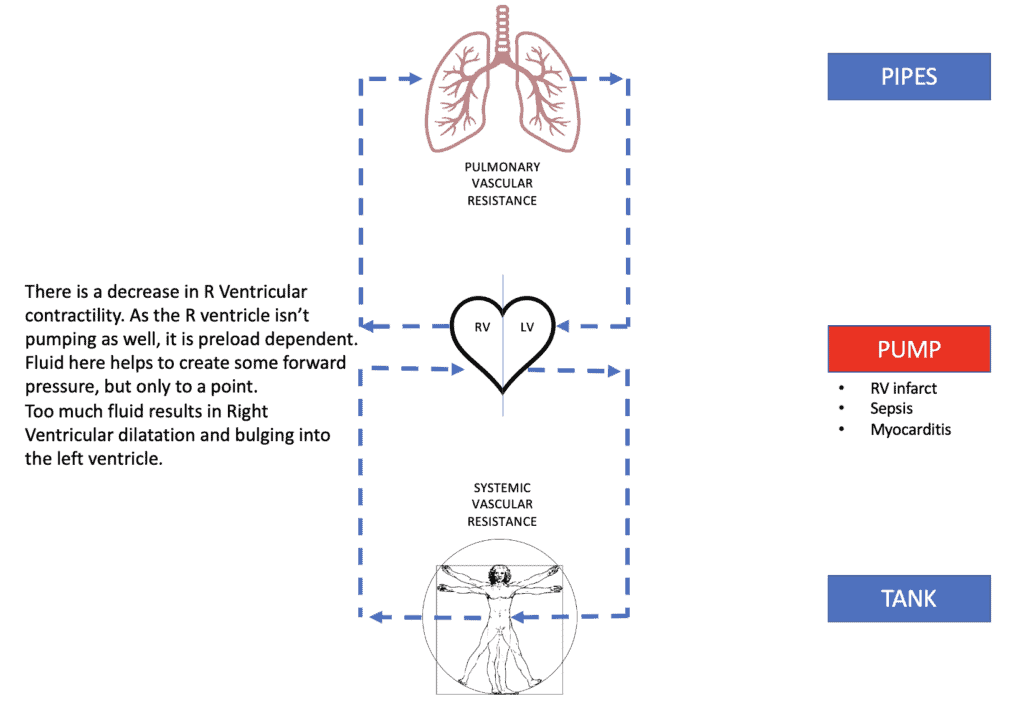
Pump, Pipes Tank: Right Ventricular Infarction
Pump, Pipes Tank: Fluid Overload

Management of Decompensated PE
The best way to return Blood pressure to normal is to reduce the clot burden. There does not need to be complete resolution of the clot, just some improvement for the haemodynamic status to improve.
The most important thing is NOT to give large volumes of fluid. A small fluid bolus of say 250ml, will not do much harm, however more than that will start the spiral.
Start inotropes or Vasopressors Early.
Adrenaline is the first line drug. The beta actions can cause pulmonary vascular dilatation and increase contractility of the right ventricle. Aim for a MAP of 65 to ensure there is right coronary artery perfusion.
Vasopressin is a second line agent causing systemic vasoconstriction and pulmonary vascular dilatation.
The next agents required are pulmonary vascular dilators, such as Nitric oxide offered by ICU. If ICU is not available, consider Nitroglycerin 5mg, nebulised.
Then specific treatment ie anticoagulation or thrombolytics or clot removal.
Oxygen is also helpful via nasal cannula, as it may assist with hypoxia and is a pulmonary artery dilator as well. Avoid positive pressure ventilation as this can further drop blood pressure.
Why patients crash during intubation and how to avoid it.
The best reason to avoid intubation in these patients is that it precipitates cardiac arrest. A significant number of cardiac arrests occur at induction. The sedative agents must be carefully chosen as they can decrease blood pressure. Beware positive pressure ventilation as well as hyperaemia and hypercarbia as they increase Right Ventricular afterload.
Aim for:
- Cardiostable Induction as with Ketamine
- Aim to increase the systolic blood pressure to at least 120-130mmHg with Adrenaline or Vasopressin, prior to intubation.
- Maintain as much oxygenation as possible, without positive pressure ventilation ie nasal prongs.








Great article thanks Dr. Kas!