Previous history includes hypertension. She is on a DOAC, and metoprolol and Perindopril.
She is haemodynamically stable.
The ambulance have given aspirin and topical GTN. On arrival she is pain-free.
Her ECG is shown below.
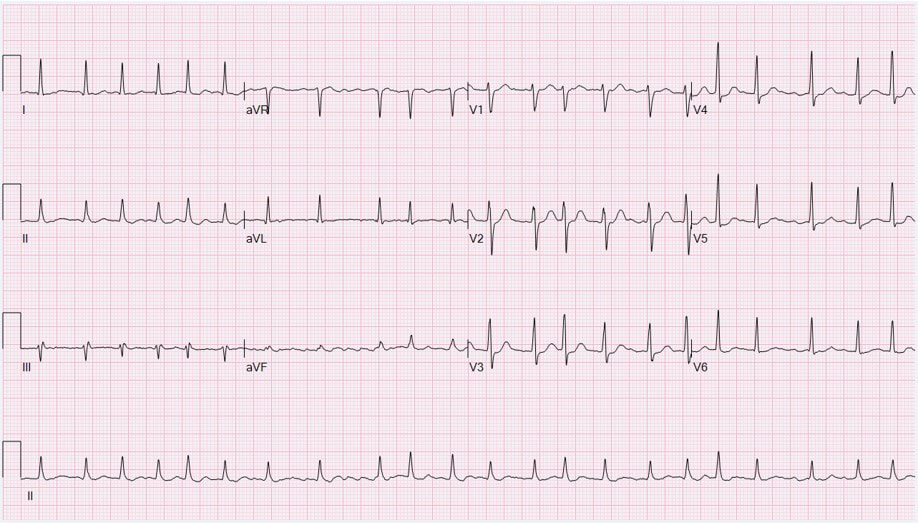
Blood tests are essentially normal, however the high sensitivity troponin is 89 ng/L (normal is <14). Is this a type I or type II Myocardial Injury(MI)? Differentiating the two can sometimes be very difficult.
MI is now far easier to detect with high sensitivity troponin. Troponin are very specific for MI, however they do not really give us the cause.
Myocardial infarction is caused by coronary thrombus, however non-thrombotic causes also exist. Type II MI is due to a mismatch between oxygen supply and demand and is due to causes other than atherothrombosis including:
- Coronary artery spasm
- Coronary embolism
- Coronary artery dissection
- Other specific causes
- hypoxaemia
- anaemia
- hypotension
- severe hypertension
- Brady/tachyarrhythmias.
Differentiating between subtypes, of which there are 5, according to the 4th universal definition of MI, can be challenging.
Mortality Outcomes
Both short and long term mortality is higher in type II rather than type I MI. Predictors of poor survival in those patients with type II MI include:
- Older age
- Female
- Heart failure
- Shock
- The presence of CAD
Troponin
Those patients with Type II MI usually have a lower peak troponin level.
A 20% change in Troponin differentiates between stable and dynamic troponin patterns.
There are some recommendations that a 50% change in troponin should be used for dynamic change and a 20% change used when the baseline value is substantially elevated.
Differentiating between Types I and II can be difficult, however in general, if there are signs and symptoms of ischaemia, type I MI should be diagnosed.
These patients should all be admitted.
Reference
DeFilippis A et al. Assessment and Treatment of Patients with Type 2 Myocardial Infarction and Acute Nonischemic Myocardial Injury. Circulation 2019;140:1661-1678







