A recent clinical practice article in the NEJM(1) on Transient Ischaemic Attack (TIA) gave a nice summary of this topic.
Current guidelines that are good reference sources on stroke and TIA management include:
- American Heart Association and the American Stroke Association (AHA–ASA),(2)
- NICE,(3) and the
- European Stroke Organization(4)
Definition of TIA
The new definition of TIA is a tissue based definition, rather than a time based definition as previously. A TIA is an ischaemic episode lasting less than 60 minutes with no evidence of infarction (5). This definition therefore includes the results of imaging, because up to 50% of patients with an initial diagnosis of TIA are found to have infarctions on diffusion weighted MRI.
Think about TIA and stroke in a similar way we think about the chest pain patient. TIA is the equivalent of angina pectoris whereas stroke is the equivalent of infarction.
Clinically however, a TIA and a minor ischaemic stroke is managed in the same way.
ROSIER
Recognition of stroke in Emergency Room(ROSIER) is a validated rule for differentiating acute stroke from its mimics.
Any of the following that is new onset favours stroke:
- Assymetrical weakness of face or arm or leg
- Speech disturbance
- Visual field defect
Loss of consciousness and seizure activity, indicate stroke mimics rather than stroke.
Risk of Stroke following a TIA
The risk of stroke within 3 months of a TIA has been estimated to be as high as 20%, with the greatest risk being in the first 10 days. However the use of risk prevention strategies may have decreased this risk considerably(6).
Investigation of the TIA Patient
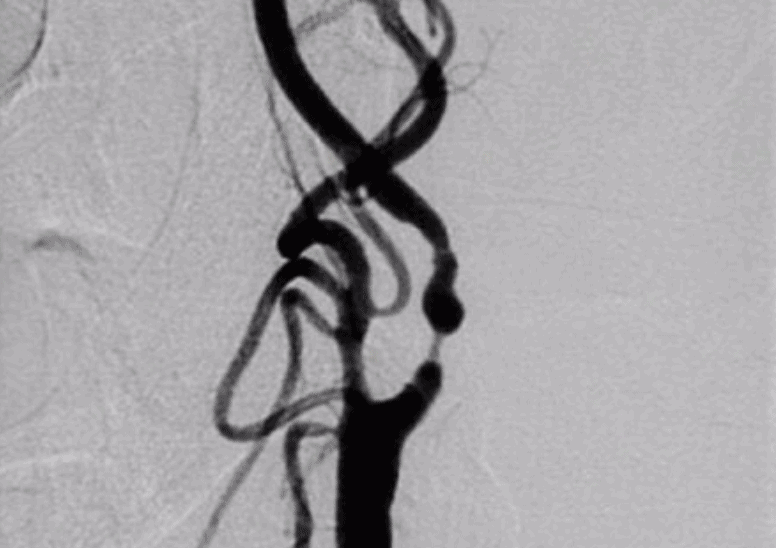
Imaging
- MRI: Diffusion weighted MRI scan is the imaging modality of choice. If this is normal and there is still a high suspicion of stroke, perfusion weighted imaging can be performed.
- CT: The NICE guidelines(3) recommend that no CT be done unless an alternative diagnosis is suspected, however a CT is probably appropriate where there is no MRI
- Extra and Intra-cranial arteries should be imaged if this will change management. This can be done by:
- Carotid Artery Ultrasound
- CT angiography, or
- Magnetic resonance angiography
Other
- ECG : determine if there is atrial fibrillation/flutter
- Cardiac Monitoring: This can be done as an inpatient, or more prolonged outpatient holter monitoring can be undertaken, to determine the presence of arrhythmia
- Trans-oesophageal echocardiography (TOE) to detect cardiac abnormalities such as:
- Patent foramen ovale
- Atrial thrombus
- Valvular Disease
- Atherosclerosis of the aortic arch
- Labs: Basic bloods should all be done. Remember to add CRP and ESR if the presentation is suggestive of temporal arteritis ie., headache and monocular blindness.
Assessing Risk
The ABCD2 score is used to assess the risk of stroke(7), especially in the first 2 days post TIA. The score ranges from 0-7 and takes into account factors of:
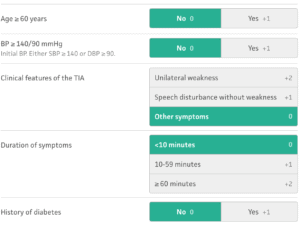
- Age
- Blood Pressure
- Clinical features of
- unilateral weakness
- speech impairment
- Duration of symptoms
- <10 minutes
- 10-59 min
- >59 minutes
- Diabetes
More recently the ABCD2-I and ABCD3-I scores have been used.
- The ABCD2-I score(8) adds the results of diffusion weighted imaging.
- The ABCD3-I score (9) adds
- a stenosis of >50% of the ipsilateral carotid artery and
- a dual TIA ie., an earlier TIA within 7 days
Should we use these ABCD scores?
The NICE guidelines recommend AGAINST using the scores as they are poor at discriminating low and high risk of stroke after TIA, when used in isolation. The addition of brain imaging modestly improves discrimination. “All cases of suspected TIA should be considered as potentially high risk for stroke”. (3)
Treatment
Aspirin
In non-cardioembolic events it decreases the rate of stroke in the first 90 days. It’s benefit beyond 90 days is uncertain.(10) Give a loading dose of 300mg oral, followed by 75-100mg daily for 90 days.
Aspirin and Clopidogrel
Combination therapy of Aspirin and Clopidogrel may further decrease the risk of major ischaemic events, however there is uncertainty about it being associated with a higher risk of major haemorrhage at 90 days than aspirin alone.(11, 12)
Oral anticoagulation
If atrial fibrillation is found, the patient needs to commence oral anticoagulation
Other treatment
- Blood Pressure control
- Lipid lowering
- Diabetes control
- Carotid Endarterectomy in those with a >50% ipsilateral carotid artery stenosis
References
- Amarento, P. Transient Ischemic Attack. NEJM May 14, 2020; 382:1933-1941
- Easton JD, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council: Council on Cardiovascular Surgery and Anesthesia: Council on Cardiovascular Radiology and Intervention: Council on Cardiovascular Nursing: and the Interdisciplinary Council on Peripheral Vascular Disease: the American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke 2009;40:2276–2293.
- National Institute for Health and Care Excellence (NICE). Stroke and transient ischaemic attack in over 16s: diagnosis and initial management. NICE guideline [NG128]. May 1, 2019(https://www.nice.org.uk/guidance/ng128.).
- European Stroke Organisation (ESO) Executive Committee, ESO Writing Committee. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis 2008;25:457–507.
- Albers GW, et al. Transient ischemic attack — proposal for a new definition. N Engl J Med 2002;347:1713–1716.
- Amarenco P, et al. One-year risk of stroke after transient ischemic attack or minor stroke. N Engl J Med 2016;374:1533–1542.
- Johnston SC, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet 2007;369:283–292.
- Giles MF, et al. Addition of brain infarction to the ABCD2 score (ABCD2I): a collaborative analysis of unpublished data on 4574 patients. Stroke 2010;41:1907–1913.
- Merwick A, et al. Addition of brain and carotid imaging to the ABCD2score to identify patients at early risk of stroke after transient ischaemic attack: a multicentre observational study. Lancet Neurol 2010;9:1060–1069.
- Rothwell PM, et al. Effects of aspirin on risk and severity of early recurrent stroke after transient ischaemic attack and ischaemic stroke: time-course analysis of randomised trials. Lancet 2016;388:365–375.
- Wang Y, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11–19.
- Johnston SC, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA. N Engl J Med 2018;379:215–225.







