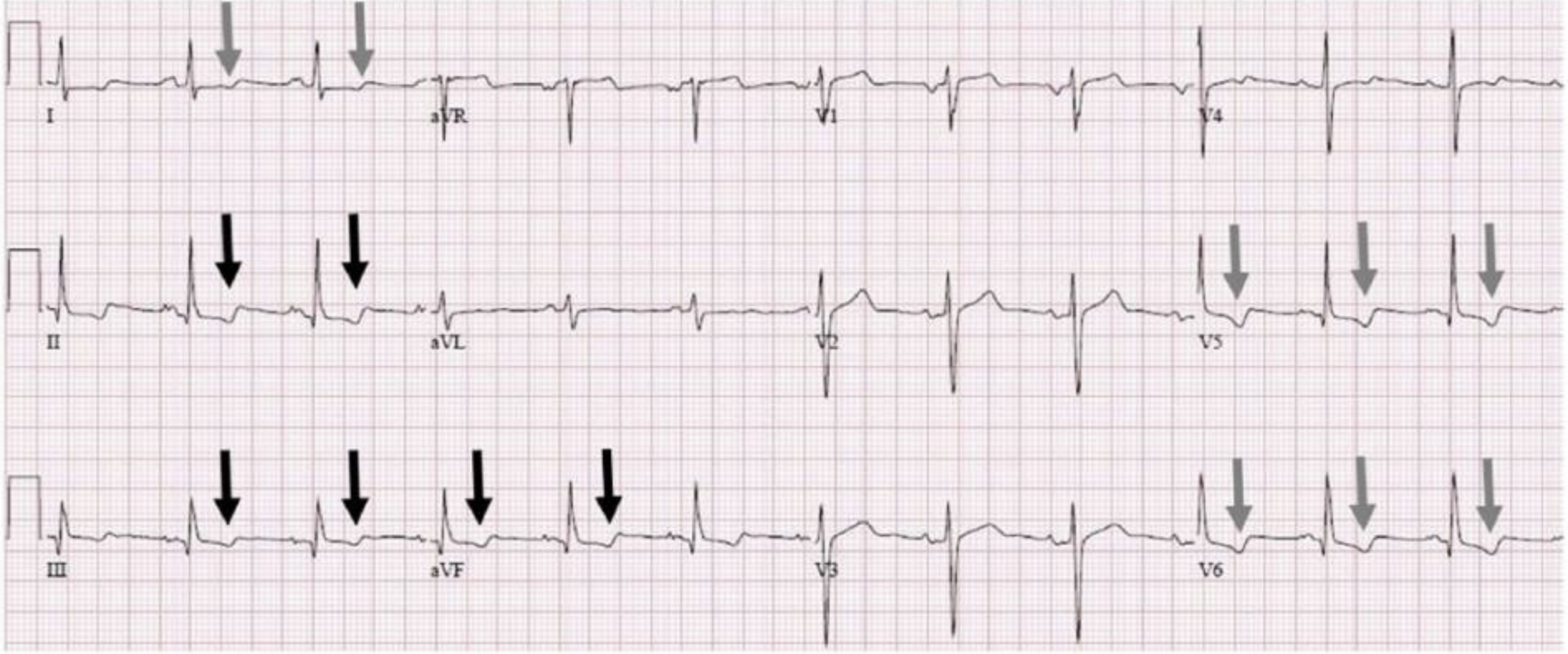
The ECG is normal except for some non-specific T wave changes in the inferior and lateral leads. What do we do with these changes? Is this inferolateral ischaemia? This patient has ECG changes so needs to be worked up as per a chest pain stratification and pathway tool. Is there anything more that we can do to work out if these changes are cardiac in origin?
What are non-specific T wave changes?
They occur in about 1% of patients and include T wave flattening and T wave inversion with no other changes necessarily present.
Causes include(1):
- Myocardial Infarction
- Myocarditis
- Mitral valve prolapse
- Ventricular Strain.
Can changes be due to respiration?
Respiration results in a change in heart position. The heart rotates in a clockwise direction in inspiration and anticlockwise in expiration. This can cause T wave changes. Inspiration also produces diaphragmatic movement, which can cause T wave changes (2)
A 2017 case report(1) looked at one case where non-specific T wave changes had a respiratory cause and recommends we look for this.
The authors recommend that:
- An ECG be performed with the breath held in deep inspiration and
- A second ECG be performed with the breath held in in expiration.
A change in the polarity of the T waves with respiration may indicate a non-cardiac cause is more likely.
The ECG below was done in inspiration.
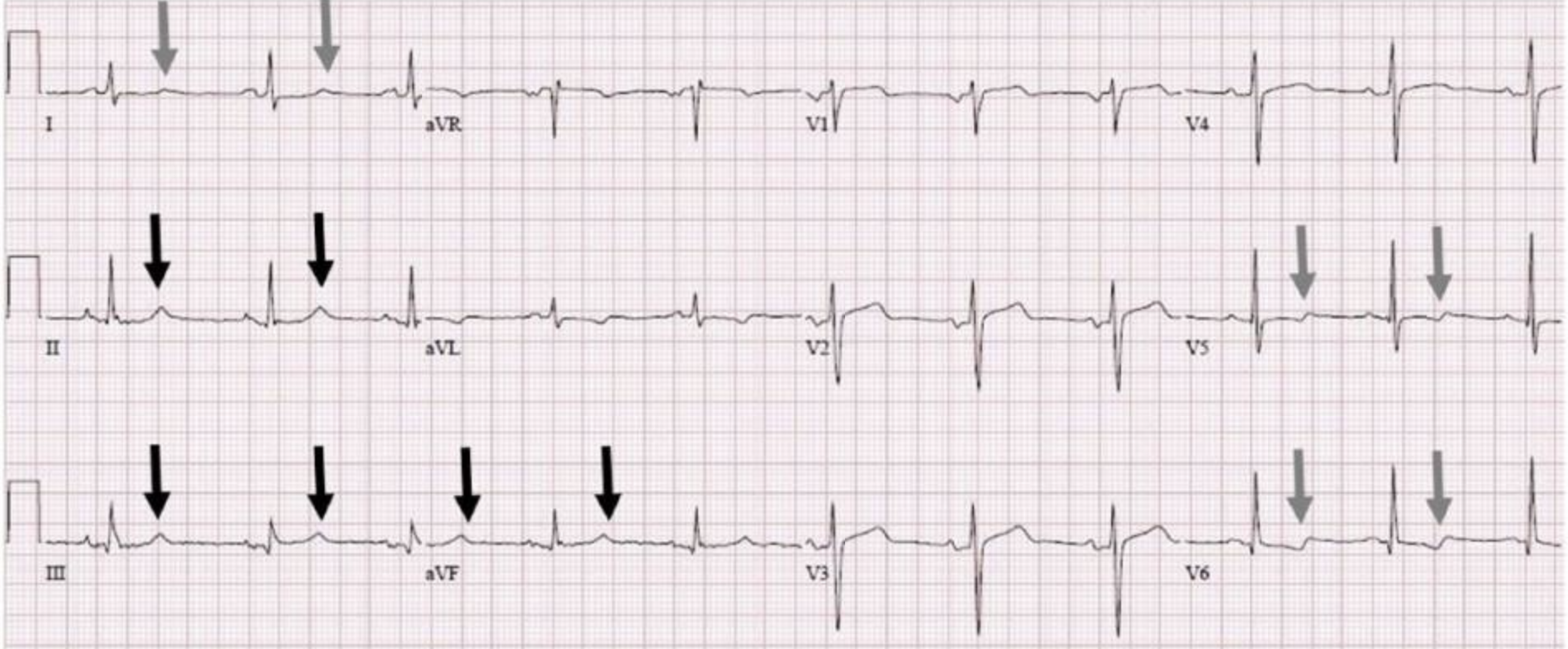
In the above ECG, the T waves in the inferior leads are now upright. The T wave morphology has also changed in the lateral leads.
This indicates a potential respiratory cause.
We must beware however, as this patient has risk factors and is not really low risk:
- If we applied a Heart Score to this patient, it would be 5 even if the troponin were normal, so a moderate risk.
- If EDACS was applied, again they are not a low risk patient.
This patient would still benefit from serial troponins and being assessed on a chest pain pathway.
References
- Sharma H and Tiwari A. Respiratory T-Wave inversion in a Patient With Chest Pain. Clinical Medicine Insights: Case reports. 2017;10: 1-3
- Dougherty JD. The relation of respiratory changes in the horizontal QRS and T-wave axes to movement of the thoracic electrodes. J Electrocardiol. 1970;3:77–86.








Peter…
Excellent presentation and discussion! Thanks!
Jerry