A 64 year old male is sent into the Emergency Department by an audiologist with a sudden, greater than 50dB hearing loss in the right ear. The patient was previously being tested for a hearing aid in the left ear, however he woke up 2 days previously with marked hearing loss in the right ear. He had not been unwell, nor had any trauma. His only previous history was of hypertension, for which he was on medication.
It’s easy to refer this patient to see an ENT at some point, but we should treat it as an emergency. If there is a cause, we need to ensure it isn’t sinister and if it’s idiopathic, we only have a small window of time to treat and potentially reverse the hearing loss. I think of this condition in terms of urgency, in the same way as I think about Temporal arteritis.
Definition of Sudden Hearing Loss
This is defined as sensorineural hearing loss(SNHL) of greater than 30dB over 3 contiguous frequencies, occurring over the previous 72 hours or less.
What causes sudden hearing loss?
In up to 90% of cases, no cause is found. However it is important to approach these patients methodically, to ensure we do not miss some of the more serious diagnoses. Here are some of the causes:
EXTERNAL EAR CANAL
- Blockage by wax or a foreign body or even by otitis externa
MIDDLE EAR
- Tympanic membrane perforation
- Haemotympanum
- Otitis media with effusion
- Cholesteatoma
- Ossicular chain pathology
- Trauma such as barotrauma or post operative
INNER EAR
- Idiopathic in 90% of cases
- Infective causes
- HIV, CMV, HSV, Mumps, Rubella, syphilis
- Autoimmune Causes
- SLE, Ulcerative Colitis
- Tumours
- Vestibular schwannoma(acoustic neuroma), leukaemia, myeloma
- Neurological
- Multiple sclerosis, stroke, migraine
- Medications
- Aminoglycosides, frusemide, NSAIDs, plus others
- Other
- Stroke, Sickle cell disease, barotrauma, perilymph fistula
An Approach to the patient with sudden hearing loss
The approach below allows us to look for most of the causes
- Was it Sudden?
Ensure that this is not a progression of hearing loss or of disease such as Meniere’s
2. Is it Unilateral or Bilateral?
Bilateral Disease is very rare. Bilateral SNHL is associated with neoplasia, vascular disorder, trauma, autoimmune disease
3. Is it conductive or SNHL
Perform the Rinne and Weber tests with a tuning fork
The Rinne test involves a 512Hz tuning fork to try and decide of conductive or not. Tap the tuning fork on your knee and hold it onto the patient’s mastoid. When the sound is no longer heard, place it 3-4cm in front of the ear.
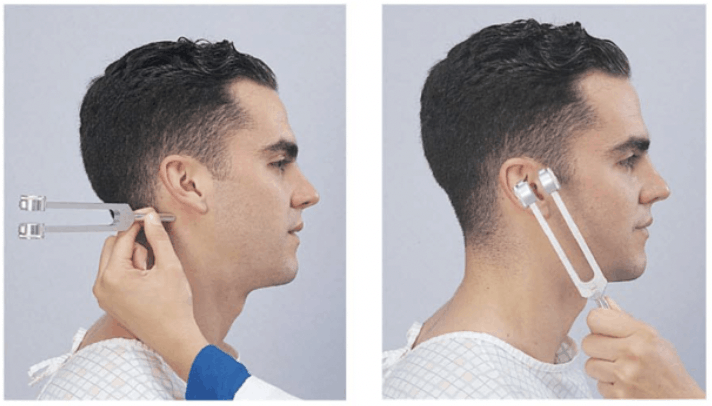
A normal test is one where the air conduction is better heard than the bone conduction ie., when the patient no longer hears the sound with the tuning fork held against the mastoid, but then hears it when placed in front of the ear.
The Weber test identifies lateralisation. Tap the tuning fork and hold it high against the middle of the forehead. In a conductive loss of one side, the sound is heard more on that side
4. Examine the ears
Examine the external auditory canal and look at the tympanic membrane
5. What does audiometry show?
If this is available, it is very helpful. Audiometry can look at the tympanic membrane mobility which gives us information on the middle ear
6. Is there other neurology?
Always perform full neurological examination. Sometimes a screening neurological examination can give us a lot.
7. Investigate as needed
Labs can include: FBC, EUC, ESR, BSL. There are many more tests that can be performed but are not necessarily emergency medicine tests.
Imaging: An MRI with contrast is the image of choice. It will give information on acoustic neuromas, demyelination and stroke.
WHAT HAPPENED TO OUR PATIENT?
- Our patient’s hearing loss was sudden
- It was unilateral
- Rinne and Weber were normal ( so most likely SNHL)
- Ear examination was normal
- Audiometry showed normal tympanic membrane mobility ie., probable normal middle ear function
- On a screening neurological examination(watch my screening examination here), the patient fell to the right on tandem gait, indicating a potential cerebellar problem.
- Bloods were essentially normal. An MRI was performed that was normal except for an old right cerebellar infarction.
MANAGEMENT OF IDIOPATHIC HEARING LOSS
If a cause is found, this can be managed as necessary. However in most cases(about 90%), as in our case, no cause was found.
Management guidelines for sudden hearing loss, stipulate that for idiopathic hearing loss, treatment with prednisolone is necessary.
A 10 day course of 60mg of Prednisolone daily was commenced. The plan was to repeat audiometry in 10 days and if the hearing had not significantly improved, then intra-tympanic steroid injections would be commenced.
There is no indication for antivirals, although some guidelines consider hyperbaric therapy as having a role.
Our patient was commenced on 60mg daily of Prednisolone for 10 days. On followup, the patient’s hearing had improved markedly.
Given that we had also found an old stroke, the patient was commenced on secondary stroke prevention medication including aspirin and anti cholesterol medication. The patient was already on antihypertensives.
References
- Coulin AE et al. Treatment of sudden sensorineural hearing loss: A systematic review. Arch Otolaryngol head and Neck Surgery 2007; 133:573-581
- Stachler RJ et al. Clinical practice guideline:sudden hearing loss. Orolaryngol head and Neck Surgery 2021;146:S1-S3







