
At Cardiac Bootcamp we look at ischaemia on ECG and go over how to differentiate it from Pericarditis or Benign Early Repolarisation.
Follow these 4 rules to increase your chances of picking up ischaemia. See the examples below.
A 38 yo patient presents with chest pain. The ECG is shown below.
Is this ischaemia, pericarditis or benign early repolarisation(BER)?
Is this ischaemia, pericarditis or benign early repolarisation(BER)?
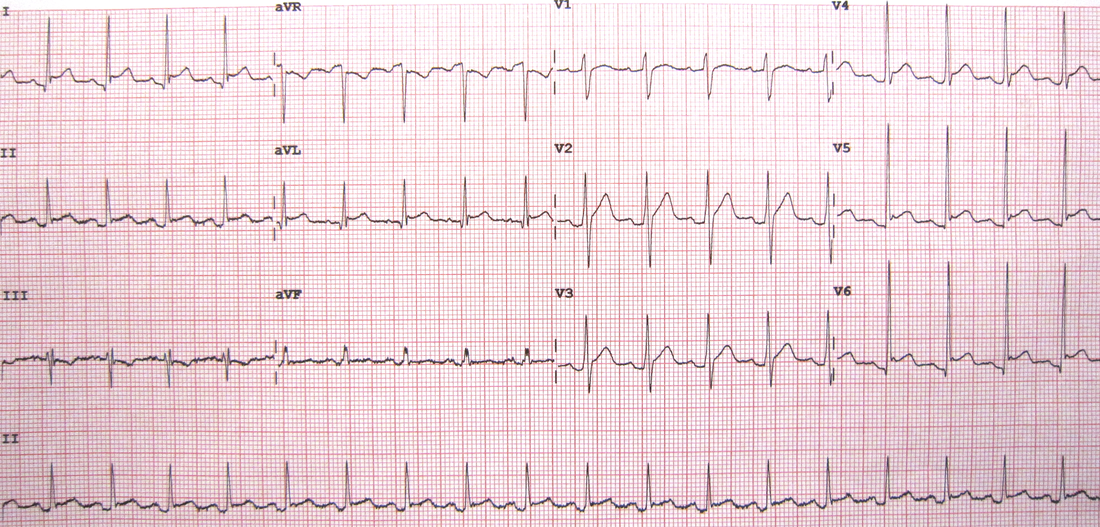
Let’s answer the 4 questions. This ECG is not a straight-forward rule in.
- Is there ST depression in any lead other than aVR and V1
- There may potentially be some ST depression in III- This could be ischaemia
- There is also some PR depression, which may point to pericarditis
- Is STE III>II
- No
- There is some STE in I, aVL, II, V4-V6- Too many territories to be ischaemia
- Is there a QRT Sign or a convex segment
- No
- Are there hyperacute T waves
- No
This is probably not an ischaemic ECG. Can we rule in Pericarditis or BER next?
Changes that make Pericarditis more likely than BER:
- No fish hook, ie., J point, especially in V4
- (Spodick’s Sign: There is a downslope of the ST-T segment.)
- ST segment elevation/T wave in V6 is >0.25

The diagnosis is pericarditis.







