Below is a case of a 60 yo patient with palpitations, who is commenced on a NOAC, with 8 MCQ questions that address the anticoagulation management of atrial fibrillation/flutter. Try them.
CASE
A 60 yo male presents to the Emergency Department with palpitations. He has had palpitations in the past. On a recent presentation to the emergency department, with the same complaint, the patient was found to be in atrial fibrillation, which self reverted within 9 hours of commencement.
His only past medical history is hypertension.
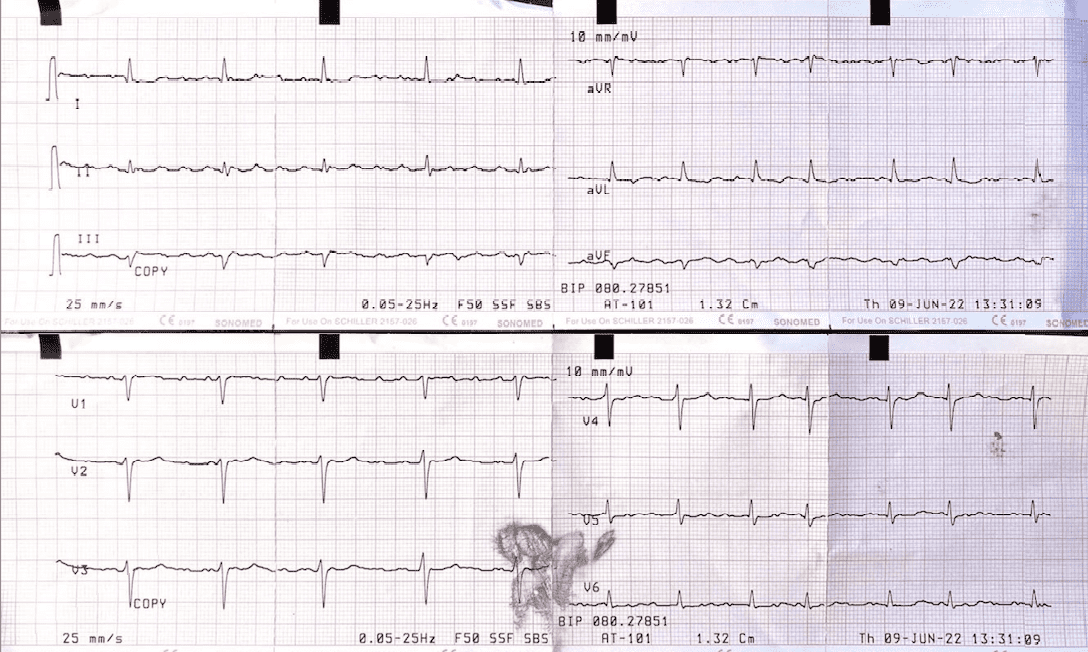
His ECG is shown below.

Q1. What does the ECG show?
(a) Sinus Tachycardia
(b) Atrial Fibrillation
(c) Atrial Flutter
(d) AV Nodal Re-entry Tachycardia
Answer
c. Atrial Flutter

Q2. You send the ECG to the Cardiologist on call. Cardiology recommend that you perform a Lewis Lead/ECG. What does a Lewis Lead ECG do?
(a) It allows differentiation between AVNRT and AVRT
(b) It detects atrial activity
(c) It allows the diagnosis of long QT to be made
(d) All of the above
Answer
b. The Lewis Lead detects atrial activity. It is used when P wave may not be readily seen.
It is especially useful in:
- Slow rhythms where the P waves will help differentiate a high grad block
- In wide complex tachycardias, where a regular P wave will exclude VT
- In Atrial Flutter, where the p waves may not all be seen.
For a review of the Lewis Lead, go to The Lewis Lead
Q3. You diagnose Atrial Flutter. What is the best option from those shown below to treat this arrhythmia?
(a) Vagal Manoeuvres
(b) Adenosine
(c) Potassium
(d) DC Cardioversion
Answer
d. DC Cardioversion, usually at 100J will be adequate to cardiovert. A lower energy level is required to revert atrial fibrillation, which is the most resistant arrhythmia and usually requires 200J.
Vagal Manoeuvres do not usually revert atrial flutter, even though they may be effective against SVT.
Adenosine will block the AV node and thus block ventricular response, uncovering the P waves.
Q4. The atrial flutter is treated. Given the patient’s history of atrial fibrillation, should the patient be anticoagulated?
(a) No as the episode of atrial fibrillation lasted less than 24 hours
(b) No as the atrial flutter is reverted and he has no stroke risk.
(c) Yes as the patient’s CHAD2DS2VASc score is > 1
(d) Yes but only if the patient has diabetes
Answer
c. The patient has hypertension and thus scores 1 on CHAD2DS2VASc, so will probably need long term anticoagulation.
Q5. The patient represents to the Emergency Department 3 weeks later, at 2pm, for an unrelated reason. Following the previous presentation, he was cardioverted and commenced on Apixaban. He has forgotten to take his morning 7am dose of Apixaban. It is now 5 hours, since he was due to take his dose. He asks what he should do?
(a) Do not take the NOAC, but take a bridging dose of enoxaparin
(b) Do not take the dose, but double the next dose.
(c) Take the missed dose immediately.
(d) Change the NOAC to a single daily dose medication
Answer
c. As per the 2021 European Heart Rhythm Practical guide on Non-Vitamin K management of ainticoagulated patients Europe (2021) 23, 1612-1675
Q6. In general, which of those shown below is a definite contraindication to a NOAC?
(a) Mild Aortic Stenosis
(b) Moderate to Severe mitral regurgitation
(c) A bio prosthetic valve
(d) A transcatheter aortic valve implantation
Answer
b.
Q7. The same patient presents to the emergency department 1 month later, still on Apixaban. His complaint is a toothache with a swollen jawline. You diagnose a tooth abscess and commence antibiotics. You refer him back to his dentist for a tooth extraction. In which of the following cases should NOACs be withheld?
(a) Simple Tooth Extraction
(b) Endoscopy
(c) Liver Biopsy
(d) All of the above
Answer
c.
Minor risk interventions include:
- Dental extraction(1-3 teeth)
- Periodontal surgery
- Implant positioning
- Cataract intervention
- Endoscopy without biopsy
- Superficial surgery- abscess incision, skin biopsy
- Pacemaker and ICD implantation
- Electrophysiological study or catheter ablation
- Routine elective coronary intervention
- IM injection
Q8. The same patient presents to the emergency department 3 months later, still on Apixaban. He has a severe headache. A CT reveals an intracranial haemorrhage. Whish of the following is correct?
(a) Immediate reversal with Idarucizumab 5mg IV is needed which can be given as two consecutive infusions of 2.5mgIV over 5 minutes( or as bolus)
(b) Fresh Frozen Plasma
(c) Andexanet Alpha at 400mg (at 30mg/min) bolus, followed by an infusion
(d) Coagulation factors VII IX, X, must be given
Answer
c.
Idarucizumab is for Dabigatran reversal.
FFP does not work as well and Coagulation factors don’t need to be given.
REFERENCE
Steffel J et al. 2021 European Heart Rhythm Association Practical Guide on the Use of Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation. Europe (2021) 23, 1612-1676.







