
Upper Gastrointestinal bleeding (UGIB) affects approximately 1 in 1000 of the population per year and has an overall mortality of up to 10%.
The cause of the UGIB in the patient in front of you may not be known, however a targeted history related to medication and alcohol use, can help with making a diagnosis in the undifferentiated patient. Ulcers are the most common cause of UGIB and they may be secondary to H. pylori infection or NSAID use. Clinically it may be difficult to distinguish them from gastric erosions, which are mostly related to alcohol and NSAID use. Other causes of UGIB include mucosal tears (Mallory-Weiss tear)which are usually associated with vomiting and gastric cancers. In patients with alcoholic liver disease and portal hypertension, we need to be suspicious that this is a variceal bleeds.
In the patient who presents with haematochezia, an UGIB should still be in our differential.
…….. But what about that patient who is vomiting frank blood and needs resuscitation. We may not have much information on past history…. and at that point it doesn’t matter. We need to RESUSCITATE.
Resuscitation of the Massive GI Bleed.
No real definition of what constitutes a massive UGIB exists. However we recognise that patient because they are unstable on the background of haematemesis, or other signs of UGIB. Sometimes instability can be subtle. It can be a relative tachycardia or a high shock index. Medications such as beta blockers (which patients with cirrhosis and portal hypertension) can mask tachycardias.
This is the patient where don’t have time to wait for the haemoglobin to return, or practice a restrictive blood transfusion policy. This is the patient who probably needs blood now….. You get the idea.
Resuscitation
- Ensure the airway is intact. Some patients will need intubation, not only for ongoing haematemesis and aspiration risk, but also for decreased levels of consciousness (hepatic encephalopathy). However as you would expect intubation will be difficult, firstly from the procedure point of view with blood obscuring the field of vision and secondly in terms of physiology and the risk these patients have of peri/post intubation cardiac arrest.
- Nurse the patient head-up and if possible intubate in the head-up position.
- 2 large bore IV cannulas: Take blood at this point for basic tests including coagulation. Send off for X-match and G&H.
- Give crystalloid, but avoid giving too much. 1L of crystalloid, perhaps 1.5L is more than enough before blood is needed.
When to give blood products?
Start blood products early. You may need to initiate the massive transfusion protocol (MTP) in your hospital. Your institution will have its own MTP design, however it is usually packed red blood cells:FFP:Platelets at a 1:1:1 ratio. If there is a delay in initiating this and the patient is not responding to crystalloid we need to give uncrossmatched blood.
Patients with a platelet count < 50,000 uL and active bleeding, should receive platelets. These will be part of a MTP. However in patients with cirrhosis and a variceal bleed, increases in platelet counts may be temporary and more are needed.
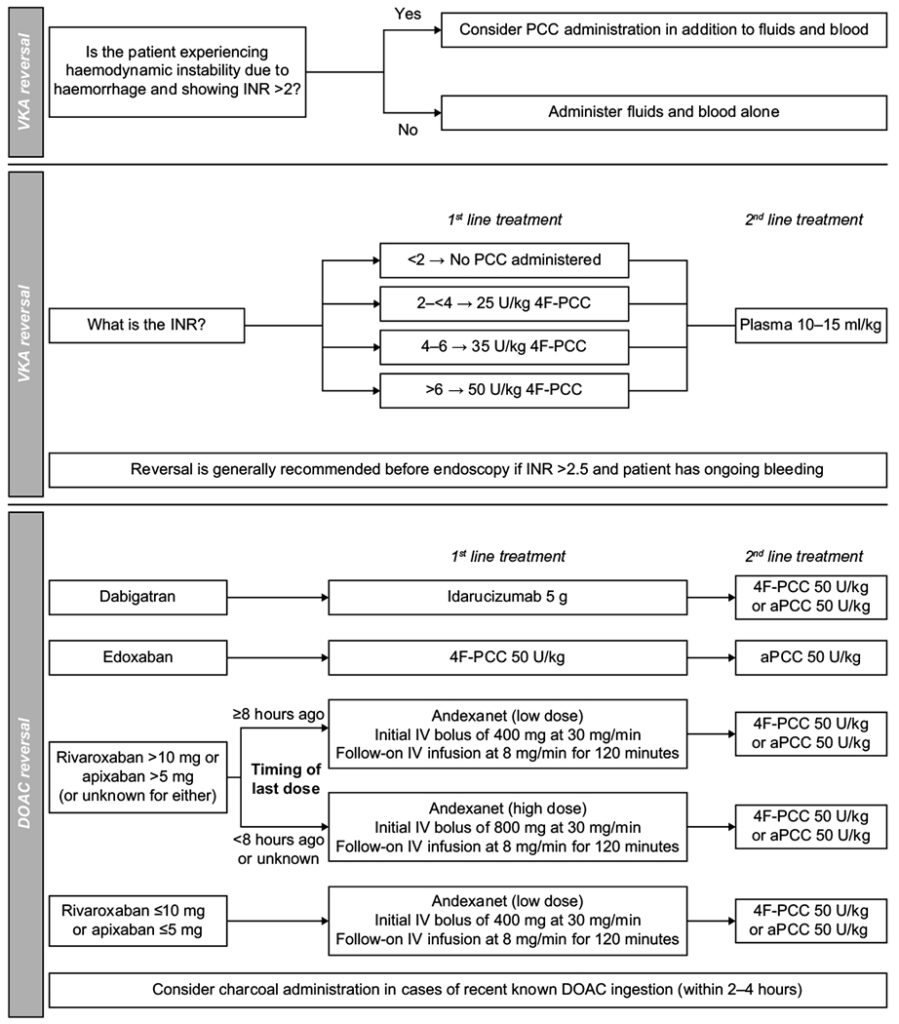
Reversing Anticoagulation
In stable patients we need to determine why the patient is on anticoagulants and then look at the risk versus benefit of reversing them. In unstable patients who need resuscitation for ongoing bleeding, anticoagulation should be reversed. We should always include haematology in these discussions.
High risk conditions such as mechanical valves, need early resumption of anticoagulation and expert haematology opinion must be sought, due to the scarcity of high quality studies to guide us.
Goal INR is 1.5-2.5
In cirrhosis, the INR may be raised and may not be an indicator of coagulopathy. Consider TEG/ROTEM to assist with what factors are needed.
Increased INR > 2
- 4 factor prothombinex complex concentrate (PCC) 25 -50 U/kg
- Give Fresh frozen Plasma (FFP) if no PCC available. 4-6 units IV
Target specific DOAC reversal agents are also available for factor Xa inhibitors (Andexanet alfa) and Dabigatran IIdarucizumab).
Below is a table of recommended reversals(5)
 Above are our priorities for our unstable patient. There are many other interventions shown below and they should be given, however in most cases they are helpful to the endoscopist and cannot take priority to the medications above.
Above are our priorities for our unstable patient. There are many other interventions shown below and they should be given, however in most cases they are helpful to the endoscopist and cannot take priority to the medications above.
Proton-Pump Inhibitors (PPI)
Current recommendation: Pantoprazole or esomeprazole 80mg IV bolus then infusion of 8 mg/hour for 72 hours. This primarily assists in patients with non-variceal bleeding, however if we are uncertain of the aetiology it can be given.
In a Cochrane systematic review and meta analysis it was found that PPI pre-endoscopy did not reduce mortality, rebleeding or the need for surgery. What PPIs do is decrease the number of ulcers with high risk stigmata at endoscopy. It is important to give the PPI, however it does not take precedence over blood products.
Antibiotics
Prokinetics agents empty the stomach of retained blood or clots and improve endoscopic visualization. Erythromycin 250 mg over 90 minutes before endoscopy, does not change clinical outcomes, but improves the views for the endoscopist and reduces the need for repeat endoscopy. Beware giving this in patients with prolonged QT interval.
Cephalosporins decrease mortality in undifferentiated bleeds. They are aimed at patients with cirrhosis and are prophylactic against subsequent sepsis. We can give Ceftriaxone 1g IV, or if there is a known allergy to cephalosporins we can use Ciprofloxacin. NNT for mortality = 22.
Octreotide
This is a somatostatin analog, which decreases splanchnic blood flow. It is recommended for used in known cirrhosis, however can be used if we are uncertain of the aetiology of the bleed. The dose is a 50mcg bolus then an infusion of 25-50 mcg/hr. The bolus may be repeated in the first hour if bleeding is not stopped. It decreases the need for blood and surgery, but has no effect on mortality in undifferentiated UGIB.
Tranexamic Acid
No place for use in UGIB. The HALT-IT trial (reviewed in papercut) was RDBPC trial with 12009 patients. They gave 1g IV over 10 minutes and then an infusion of 125 mg/hr for 24 hours. They found no difference in mortality reduction at 5 days, or mortality reduction at 28 days between TXA and placebo, plus there was a slight increase in seizures and venous thromboembolism in the TXA group.
Sengstaken-Blakemore Tube
Balloon tamponade can be used for bleeding oesophageal or gastric varices, not responding to medical management. It has a high initial haemostatis rate and low complication rate, but rebleeding and mortality are high.
It is contraindicated in known oesophageal strictures, or recent gastroesophageal surgery.
PROCEDURE
- Inflate gastric balloon before insertion
- Note pressures every 50 – 100mL
- Deflate and clamp ports
- Measure depth needed, but > 50cm
- Insert and inflate gastric balloon only
- If pressure > 15 mmHg above previous measurement STOP
- When in position use traction
- If bleeding does not stop inflate the oesophageal balloon
- Inflate to 30-40 mHG
- When Bleeding controlled after 3 hrs decrease pressure by 5mmHg
Conclusion
The key, the thing that makes the difference is our resuscitation; airway, breathing and circulation. Giving fluids, blood and reversing anticoagulation are the key. All the other things are also important and must be done, but cannot interfere with the initial resuscitation.
Watch the video Minutes to Mastery Lecture on EM Mastery.
References
- Fallah MA, et al. Acute gastrointestinal bleeding. Med Clin North Am. 2000 Sep. 84(5):1183-208
- Elmunzer BJ, et al. Systematic review of the predictors of recurrent hemorrhage after endoscopic hemostatic therapy for bleeding peptic ulcers. Am J Gastroenterol. 2008 Oct. 103(10):2625-32; quiz 2633.
- Bornman PC, et al Importance of hypovolaemic shock and endoscopic signs in predicting recurrent haemorrhage from peptic ulceration: a prospective evaluation. Br Med J (Clin Res Ed). 1985 Jul 27. 291(6490):245-7.
- Villanueva C, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013 Jan 3. 368(1):11-21.
- Milling TJ metal. Anticoagulant Reversal in Gastrointestinal Bleeding: Review of Treatment Guidelines. Dig Dis Sci 2012;66:3698-3714.
- Sreedharan A, et al. Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2010 Jul 7.
- Huda S et al. Management of Life-Threatening Bleeding in Patients with mechanical Heart Valves. Cureus 2021 Jun; 13(6) e15619
- Choi J Y et al. Outcomes of patients treated with Sengstaken-Blakemore tube for uncontrolled variceal haemorrhage. Korean J Int Med. 2018;33:696-704
- Keung CY. et al. Survival outcomes and predictors of mortality, re-bleeding nd complications for acute severe variceal bleeding requiring balloon tamponade. World J Heat 2022:14:1584-1597.







