We often see patients presenting with SVT. They often have ST changes, so we have to ask;
Is SVT an ischaemic arrhythmia? The answer is no, but beware as it can trigger ischaemia. Let’s look at some cases.
ST segment depression occurs during supraventricular tachycardias but is transient and usually resolves following conversion to sinus rhythm. In some cases it can persist for some time.
Patients with SVT can also have troponin leaks. Are these significant? For the most part the answer is no.
ST elevation, is usually present in aVR and this is normal in cases of SVT as shown below. For a greater explanation of SVT go to the Cardiac Bootcamp Self Study Course for members.
A few points to remember:
- ST depression and Troponin leaks occur in a significant number of patients with SVT.
- ST depression and Troponin leaks are not markers of coronary artery disease
- ST depression plus Troponin leaks plus chest pain are more prevalent in those with coronary artery disease.
So ST depression and troponin leak are OKAY, but beware if there is chest pain. It could be the SVT provoking ischaemia.
Now we’ve seen that ST elevation is fine in aVR. How about ST elevation elsewhere?
Here is a great case from the literature.
CASE
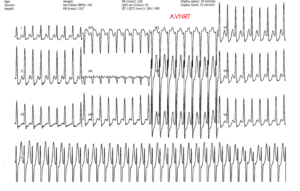
A 21-year-old male with history of hypertension and asthma presents to the emergency department with a one hour history of sudden onset of severe sternal chest pain The chest pain was accompanied by diaphoresis and shortness of breath. He felt his heart racing and became dizzy. An ECG was done:
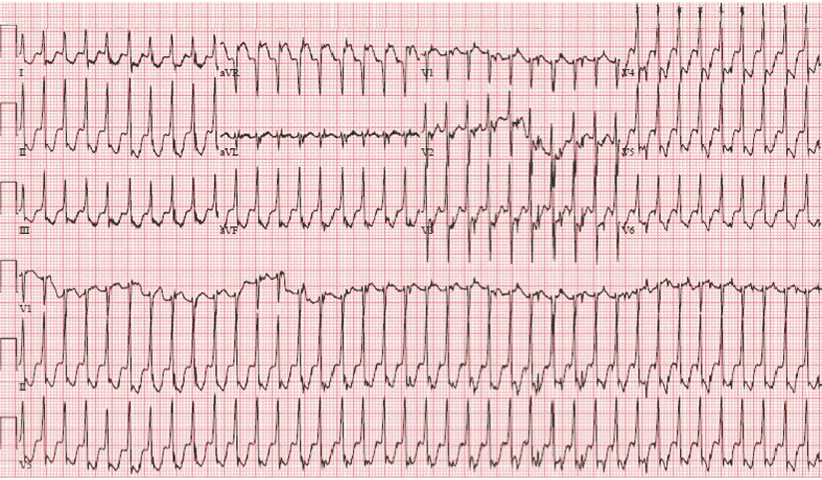
We can see that this is a rate of about 220 bpm with ST elevation in aVR and diffuse ST depression.
The patient spontaneously reverted to sinus rhythm, however the chest pain did not resolve. A post resolution ECG was done and is shown below. What do you think?
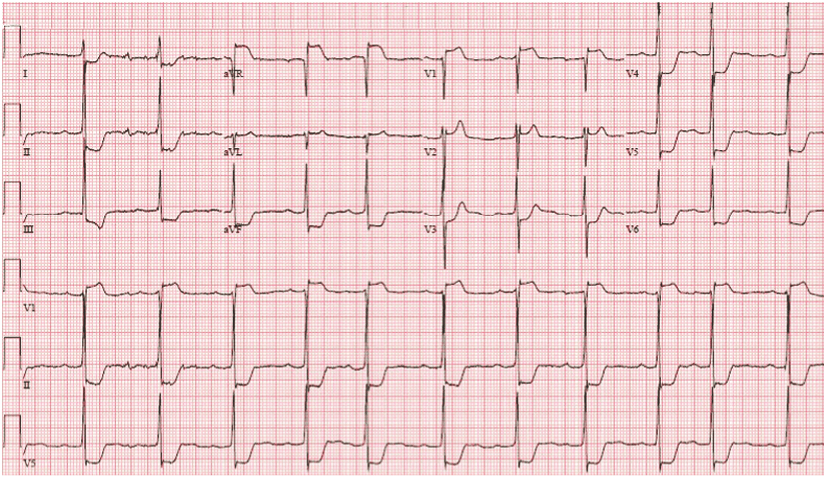
The ECG shows ST elevation in aVR and V1 and V2. There is also significant ST depression in multiple leads.
Is this a ST elevation MI? Remember the pain was ongoing. Usually ST elevation in aVR and V1 with other ST depressions may indicate a proximal LAD lesion.
What would you do?
In this case the cath lab was activated. The patient had normal coronary arteries and a left ventricular ejection fraction of 70%. There was no dissection of the ascending aorta.
The troponin was elevated. The ECG resolved and was normal by the next day.
Conclusion:
ST depression and a Troponin leak are not unusual in SVT. However chest pain may signify a different patient group, ie., those with coronary artery disease. ST elevation, other than in aVR, should always be a cause for concern.
References
- Zellweger M J et al. Elevated troponin levels in absence of coronary artery disease after supraventricular tachycardia. Swiss Medical Weekly, vol. 133, no. 31-32, pp. 439–441, 2003.
- Carlberg D J et al. Serum troponin testing in patients with paroxysmal supraventricular tachycardia: Outcome after ED care. Am J Emerg Med, vol. 29, no. 5, pp. 545–548, 2011.
- Bukkapatnam RN, et al. Relationship of myocardial ischemia and injury to coronary artery disease in patients with supraventricular tachycardia. Am J Cardiol. 2010;106:374-377.








normal block