Here is a quick review of how we are approaching intubation of potential COVID-19 patients at our hospital. Please develop your own strategy and base it on your resources. The evidence for a lot of what is done is consensus-based. There is a lot of material coming out. Here is a quick summary.
A new paper in pre-print at the moment is a good place to start.
Brewster D J et al Consensus Statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group. MJA Preprint only
We need to remember that we have to do things somewhat differently and that’s when mistakes occur as our normal approach is ingrained and almost automatic. There is a fine line between making some changes that will work and assist the patient and minimise the chances of our contamination and trying to do too many different things that will potentially lead to errors. The secret, regardless, is practice.
I think of the patients that we treat with COVID-19 to be of 3 types:
- The patient who is sick on the ward and requires to be intubated
- The person who comes into ED, with low sats and not responding to oxygen and needs intubation
- The cardiac arrest with potential COVID-19
I now consider any patient presenting to the Emergency Department as being a potential COVID-19 patient.
THE CARDIAC ARREST PATIENT
My views on the cardiac arrests without COVID-19 are that we resuscitate with no airway, except BVM until ROSC occurs ie., CPR only and BVM.
This is REVERSED in COVID-19. Intubate first and then CPR, otherwise every compression of the thoracic cage, results in potential virus being expelled. All of these resuscitations are performed with full PPE. PPE first, airway second and CPR third. It will be stressful as we want to jump in and resuscitate, but the key here is to stop and put on PPE.
Before I outline our intubation approach, I wanted to share a list some of the phrases that become important in this environment:
- SLOW DOWN, DON’T RUSH, THINK
- Rushing is when errors occur. We’re used to jumping in and taking action. Now is the time to think and prepare, so we can treat the patient and be safe ourselves, to allow us to treat a whole lot of other patients.
- PPE ALWAYS
- No short-cuts
- No saying, I’m just going into the room for 5 seconds
- Have a spotter or a buddy system to help with doffing your PPE
- PRE-BRIEF
- Ensure all staff know what is going to happen with sick patients
- COGNITIVE AIDS
- Use lists to minimise errors
- CLOSE THE LOOP IN COMMUNICATION
- Let everyone know what is happening next and ensure everyone gives feedback on when the step is completed.
- DEBRIEF
- Learn from every scenario
- PRACTICE PRACTICE PRACTICE
INTUBATION APPROACH
In our hospital we are looking at potential intubation teams, with the most experienced anaesthetists and airway nurses, providing the service. I think it’s a good approach, because the most experienced person should intubate. This is not the time to be protective and insist that we can do this. The most experienced operator does the procedure.
When looking at this, think of the potential things that can go wrong, ie., the 3am scenario when the anaesthetist that is on call is in theatre with an emergency laparotomy due to a trauma and a pre-respiratory arrest patient with potential COVID infection needs intubation.
All staff including the ED staff, must be trained in this procedure. The ED nurses must have the same level of training. The senior ED doctors must be part of the process.
SETUP
We have a very simple setup with equipment already assembled outside the room, and medications to be pre-drawn as per our flow chart.
We have 3 people in the room in full PPE (we aim to minimise the number of people in the room):
- Airway Operator: Intubates
- Airway Assistant: Hands ett and ensures no contamination by simple things such as suction etc.
- Team Leader/ Drugs etc.: Gives medications. Keeps an eye on the whole process and if something else is required, may communicate to the outside person. The hope is that all will be in place and pre-prepared.
We have one person outside the room also in full PPE. They may need to get things for us.
Our goal would be to perform the intubation in a negative pressure room, however we don’t have this, so we have to use a room that’s clean and easy to do a terminal clean on. That may be your resuscitation room. if so, think about decluttering and ensuring things are packed away.
PREPARATION
We have a brief discussion of what is to happen and then the team perform their allocated tasks.
Equipment
Most of our equipment is pre-prepared in a resuscitation box outside the room we are to intubate in.
- PPE: We have packs with gown and gloves, face mask, cap, and full face shield and I would use sealed goggles under face shield, if they didn’t push the face shield forward.
- Intubation Equipment
- Video Laryngoscope
- Endotracheal tubes(ett)
- We have 3 sizes , 6, 7 and 8
- Sizes 7 and 8 are for female and male patients respectively
- Size 6 is for a surgical airway
- Bougie
- Prepare closed circuit suction, with filter and ETCO2 (see below)
- Remember the filter should be as close to the ett as possible
- Set up the ventilator as per the ARDSNET protocol
- Nasogastric tube
- Syringe pumps etc
- We have a simple surgical airway approach which is scalpel, bougie and size 6 tube.
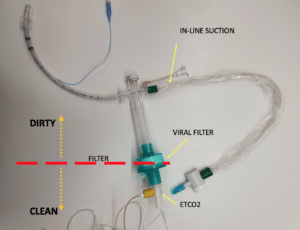
Closed Circuit suction, with viral filter as distal as possible.
Medications
- Induction: Ketamine 1mg/kg IV- we use a slightly lower dose of ketamine especially in sepsis. I know that ketamine may increase BP, but in sepsis, it can drop it. We may also use ketamine to assist in managing those combative patients that don’t keep their oxygenation on.
- Paralysis: Rocuronium 1.2-1.6mg/kg(ideal weight). We standardise to 100mcg IV for every adult patient Suxamethonium 1.5-2mg/kg (actual weight) consider giving 200mcg IV.
- My preference here is ROCURONIUM because I want a prolonged paralysis
- Blood Pressure Control: Noradrenaline infusion already drawn up for the hypotensive sepsis presentation, Metaraminol for bolus doses
- Post Intubation Sedation: We would use a stat dose of Fentanyl of 100-200mcg for analgesics purposes and then a Fentanyl infusion for sedation, or what ever you like, as long as sedation is deep here, so that the patient doesn’t gag or fight the ventilator.
- Post Intubation Continued Paralysis: A further 100mcg of Rocuronium may be needed.
INTUBATION
Pre-oxygenation
We need to take great care in pre-oxygenating patients. High flow situations can generate significant aerosols. Rebreathers and Non-Invasive Ventilation do the same thing (refer airway blog)
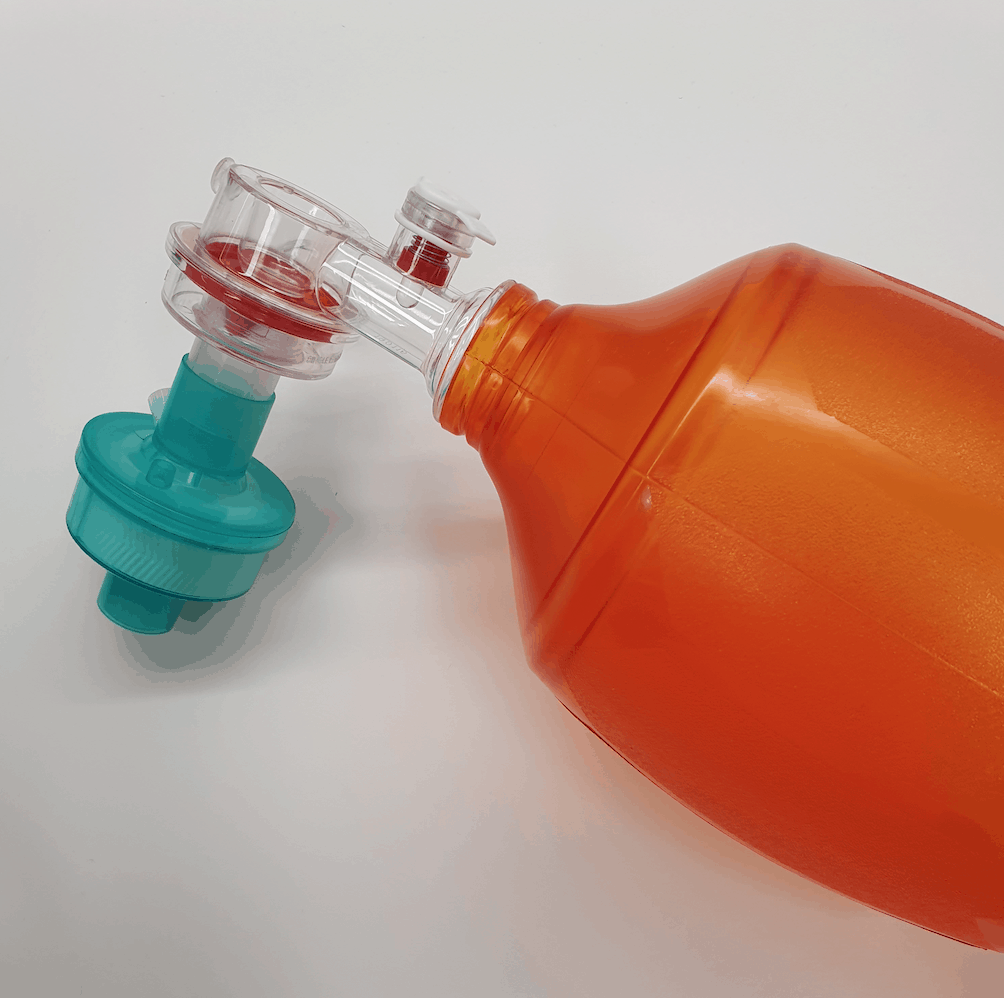
A possibility here is the use of a BVM with filter, flushed and no bagging, with the patient in a 45 degree position. Use a VICE grip rather than a claw grip, to push the mask back into the face and ensure a good seal and no leak.
There is no manual ventilation.

Induction
Ketamine 1mg/kg IV and Rocuronium 100mg IV
Wait for about 1 minute. It’s important to give a large dose of paralytic so that it has a rapid effect and to ensure that the patient is fully paralysed and doesn’t cough.
Intubation
- No cricoid as per usual.
- Video laryngoscopy
- Operator stands straight ie., doesn’t bend over to look in, ie., do NOT look into the mouth
- Bougie used.
- Railroad tube to a pre-determined depth
- 20cm for females
- 22cm for males
- CUFF UP before any ventilation( cuff pressure 26-30 cm H20) DO NOT LISTEN FOR AN AIR LEAK
- Closed suction system goes in next
- Viral filter next
- ETCO2 next
- No auscultation for tube position, use ETCO2 (refer to diagnosis of different capnography waveforms)
Is there any rescue approach?
We must be careful of rescue devices such as laryngeal masks which may cause aerosolisation. We may BVM if needed and if we get to CICO, then go to surgical airway.
Our rescue approach will be perhaps BVM with tight fitting seal, or in cases of CICO, a surgical airway. The surgical approach is vertical incision in the anterior neck, then a cut is made into the cricothyroid membrane, bougie in and then railroad size 6 ett over this. Don’t go too deep as you are at the level of the vocal cords at the cricothyroid membrane.
Post Intubation
Insert Nasogastric, NOT OROGASTRIC tube and DO NOT OPEN AND LOOK IN THE MOUTH, if there is trouble inserting. Stop and think about a re-approach with video laryngoscope in, but again do not look in the mouth.
Adequate sedation– Provide deep sedation as we want these patients to tolerate the ventilator. If there is an issue, consider paralysis for a short time until control is established.
A Noradrenaline infusion will hopefully have already been commenced in the hypotensive patient, prior to intubation. Metaraminol boluses can be used to support blood pressure until the Noradrenaline starts to work. We need to remember that a number of these patients will crash during intubation. Pre-prepare.
Ventilation: We use the ARDSNET protocol. Start on 6L/kg and then adjust PEEP and FiO2 to get saturations up. Below is a table outlining how the PEEP and FiO2 can be adjusted.
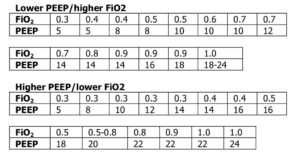
These patients respond to PEEP. Be careful post intubation. Lying the patient flat and not providing PEEPcan result in desaturation
- Start on higher PEEP after intubation (consider 5-10 of PEEP) and
- Sit the patient up at 30-45 degrees.

What about Proning?
Proning is about moving the patient onto their front to recruit more alveoli. We’ve done this in pneumonia patients, however, be careful here, as this is where you lose the tube or have disconnections. If you aren’t a centre that does this regularly, then I would probably advise against it.
The goal is to minimise any disconnections. Beware to ensure all joints are tight. If the filter is near the ett and there is a proximal disconnection, there is little contamination, however beware to not have an accidental disconnection distal to the filter.
If disconnection is needed and there is no distal filter attached. Put the ventilator on standby and clamp the tube before anything is done. Use tape on the tube to ensure that it isn’t damaged.
Ventilating Multiple Patients with one ventilator.
This is something we are talking about, however apart from a study on adult sized sheep in 2007, I’ve never seen it done. I’m not sure that I will be doing it. Below is a description of how it might be done.
A lot to talk about.
Good Luck with it.








Hi Peter and Team at Resus,
Thank you for the excellent guidance.
Regarding pre-oxygenation, knowing that manual breaths are not provided, do we have any idea how effective the described method is at delivering 100% oxygen? Single-use BVMs aren’t great when the (fatigued) patient has to generate negative pressure to take a breath.
Is there any way we can improve on this?
On it’s own the system only delivers a PEEP of 2cm H20. However if you add another section between the filter and the bag ie., an ETCO2 attachment, take the ETCO2 off it and apply oxygen at 4L it delivers 15cm H20 PEEP.
I will put these up on a McGyver section early next week.