Hyponatremia is a common electrolyte abnormality. It can be acute or chronic. It can occur in isolation or as part of other disease processes. Diagnosing its cause can be challenging in the Emergency Department and there may be some confusion over how to initially manage these patients.
Let’s clear up that confusion, with a simple 3 step process to diagnosis and a simple binary approach to treatment. But first, a short summary of the condition.
Causes
A 68 yo male presents with a past medical history of congestive cardiac failure, presents with lethargy. He is on Frusemide and Enalapril. His examination is normal except for some mild ankle swelling. He is afebrile, with HR or 79, BP 142/86 and 97% saturations on room air. His initial blood tests show a sodium of 118 mmol/L. You order full bloods and urine, which come back as follows:
- Na 117 mmol/L
- K 4.1 mmol/L
- Cl 99 mmol/L
- Urea 5.8 mmol/L
- Creat 107 micromol/L
- Serum Osmol 246 mmol/kg
- Urine Osmol 520 mmol/kg
- Urinary Na 36 mmol/L
- Gluc 6 mmol/L
What are the potential causes and how would you treat this patient in the emergency department? We will come back to this case a little later.
Definition of Hyponatremia
Hyponatremia is defined as a Na<135mmol/L. Profound Hyponatremia is Na<125mmol/L
Patient Presentation
The condition can be acute or chronic. Those patient with chronic hyponatremia can surprisingly present with few symptoms, even with very low levels of serum sodium, sometimes less than 115 mmol/L. However a rapid drop, i.e., of the same amount over 24-48 hours can result in severe cerebral oedema and brainstem herniation.
Symptoms include:
- Nausea and vomiting
- Headache
- Confusion
- depressed conscious state
- Agitated state
- Seizures
- Coma
Causes
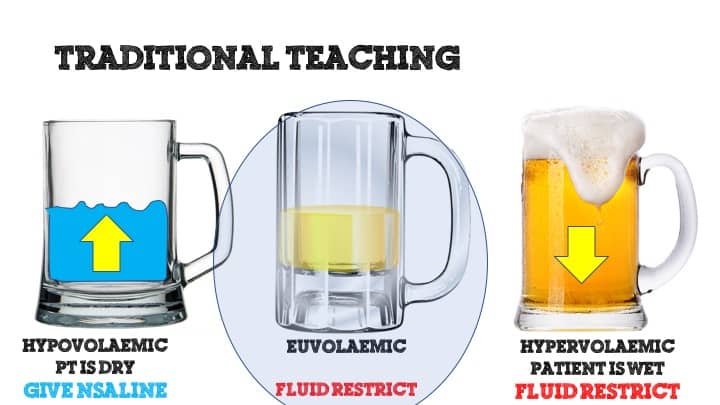
Classically patients are diagnosed according to their volume status. This may not be as easy to do as it seems on paper. It is sometimes difficult to tell euvolaemia from mild to moderate dehydration. This is is where the simplified method shown below will assist. The volume status model is still useful in looking at potential causes. Interestingly, in the literature various causes are placed in a different subcategory. For example hypothyroidism has been placed in both the hypovolaemic or the euvolaemic categories.
Hypovolaemic Hyponatremia
This occurs when sodium and free waster is lost and replaced by hypotonic fluid.
- Fluid Loss by vomiting or diarrhoea or excessive sweating, replaced by hypotonic fluid
- Renal impairment resulting in impaired water excretion
- Salt wasting nephropathy
Euvolaemic Hyponatremia
This occurs when there is normal body sodium but an excess of free water.
- Psychogenic polydipsia
- SIADH
- Cerebral Salt Wasting Syndrome: in traumatic brain injury or neurosurgical interventions. It is different to SIADH
- Drugs e.g.
- acetazolamide, thiazide diuretics, amiodarone, ACE inhibitors, carbamazepine, gabapentin, haloperidol, indomethacin, ketorolac, levetiracetam, loop diuretics, mirtazapine, opiates, oxytocin, proton pump inhibitors, SSRI, sulfonylureas, venlafaxine
- Glucocorticoid Deficiency
- Hypothyroidism
Hypervolaemic Hyponatremia
This occurs when there is an increase in total body water greater than the increase in sodium
- Acute and Chronic Renal Failure
- Cardiac Failure
- Cirrhosis
- Nephrotic Syndrome
A Simplified Approach
Treatment
As an overriding statement FLUID RESTRICT EVERYONE!
If you are certain that they are dry, dry, dry, then give them some 0.9%Normal Saline, otherwise Fluid restrict all. This is the path to causing no harm.
If they have a depressed conscious state, but not coma, or having other severe symptoms give 100ml of 3% saline over 60 minutes. This raises the Na by 2 mmol/L. You can repeat.
If they are in a coma or having a seizure, give 100ml 3% over 10 minutes. You can repeat.
BEWARE! Do not raise the serum Na by more than 8mmol over a 24 hour period as you will cause significant neurological sequelae.
Diagnosis
Diagnosing the cause of your patients hyponatremia may be straightforward. They may be overloaded, known to have cirrhosis, or they tell you they have had vomiting and diarrhoea for three days with no fluid intake. These cases are simple.
If they are not as clear cut, diagnosing may be difficult and may not be possible at presentation in the emergency department.
Take your labs which may include:
- FBC
- EUC
- LFT
- URIC ACID
- TSH
- CORTISOL
- SERUM OSMOLALITY
- URINE OSMOLALITY
- URINE NA
In those cases that aren’t clear(ie., I can’t tell dehydration from euvolaemia) cut I use my
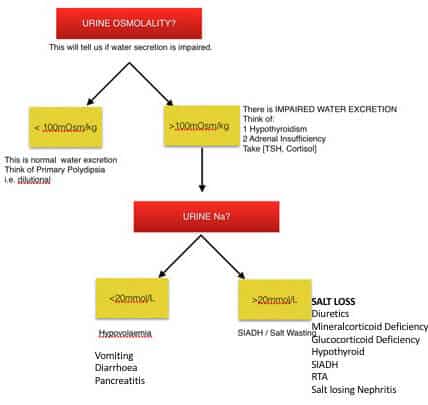
My 3 STEP approach:
- Is it real?
- Look at the serum osmolality.
- If < 290 mol/kg it is real and can proceed
- If > 290mmol/kg it is due to other proteins and may be due to hypertriglyceredaemia, or multiple myeloma etc.
- Look at the serum osmolality.
- What is the Urine Osmolality?
- Is it <100 mOsm/kg?
- This means the Urine is dilute. Probable psychogenic polydipsia
- Is it >100 mOsm/kg?
- This means that the urine is concentrated. Is this because there is more salt than water lost or less water than salt lost.
- I then look at the Urine Na
- Is it <100 mOsm/kg?
- What is the urine Na?
- Urine Na < 20mmol/L
- If the urine sodium is low and urine is concentrated, it means your patient is dehydrated with causes such as:
- dehydration secondary to vomiting, diarrhoea, third space loses
- If the urine sodium is low and urine is concentrated, it means your patient is dehydrated with causes such as:
- Urine Na > 20mmol/L
- If the urine sodium is high and the urine is concentrated, causes include:
- Salt wasting syndrome, SIADH, medications, glucocorticoid deficiency, hypothyroidism, salt losing nephritis
- If the urine sodium is high and the urine is concentrated, causes include:
- Urine Na < 20mmol/L
This may be a little simplisitic, but as a preliminary set of differentials serves the purpose.
Let’s go back to our case:
A 68 yo male presents with a past medical history of congestive cardiac failure, presents with lethargy. He is on Frusemide and Enalapril. His examination is normal except for some mild ankle swelling. He is afebrile, with HR or 79, BP 142/86 and 97% saturations on room air. His initial blood tests show a sodium of 118 mmol/L. You order full bloods and urine, which come back as follows:
- Na 117 mmol/L
- K 4.1 mmol/L
- Cl 99 mmol/L
- Urea 5.8 mmol/L
- Creat 107 micromol/L
- Serum Osmol 246 mmol/kg
- Urine Osmol 520 mmol/kg
- Urinary Na 36 mmol/L
- Gluc 6 mmol/L
What is the Treatment?
You would fluid restrict this patient, until you knew more.
Let’s look at potential causes: Use the 3 step process:
- Is it real?- Yes as the serum osmolality is <290 mmol/L
- What is the Urine osmolality? – It is high
- What is the urine Na? It is high, so the osmolality is due to a loss of Na. The potential causes are:
- Salt wasting syndrome
- SIADH
- Glucocorticoid deficiency,
- Hypothyroidism,
- Salt losing nephritis
- Diuretics
- Thiazides tend to cause hyponatraemia
- Loop diuretics tend to cause hypovolaemia
In this case, the patient is on a loop diuretic, which doesn’t tend to cause hyponatremia. He is on an ACE inhibitor, which can cause, it, but has been on this for some time.
His bloods were all run and the working diagnosis was SIADH. Remember SIADH is a diagnosis of exclusion. Synacthen test was negative, so a diagnosis of salt wasting syndrome was made.
I hope that helps.
Let me know if you’ve had some cases of this or can modify this even more so others can use.
Peter Kas








[…] Go to the blog for a full review of Hypernatraemia and Hyponatraemia. […]
Hyponatremia – Resus
hqkwkejvc http://www.g9a4b460r7yoxe27ek7jp2d7133cic82s.org/
ahqkwkejvc
[url=http://www.g9a4b460r7yoxe27ek7jp2d7133cic82s.org/]uhqkwkejvc[/url]