Epicardial fat necrosis is a rare, benign, self limiting condition that can mimic more serious causes of chest pain.
Case
A 30 yo patient presents via ambulance with a complaint of chest pain. The chest pain started at 2am in the morning and lasted all night. It was relieved with Aspirin and GTN given by the ambulance. The patient arrived in the Emergency Department 8.5 hours later.
The pain was described as central and radiating to the left arm and left jaw. It had both a pressing feeling and a pleuritic component. It was worst on lying down.
There was no relevant past history except smoking and daily alcohol intake.
History and Examination
The patient was afebrile, with normal BP however there was a sinus tachycardia of 110 bpm. The examination was normal, with dual heart sounds, chest clear, abdo soft, warm, well perfused peripheries. The pain was not reproducible on palpation.
 This patients’s ECG (ECG shown is similar to patient’s) showed a sinus tachycardia, with no ischaemic changes and apart from the tachycardia, no changes consistent with a pulmonary embolism(PE), or pericarditis.
This patients’s ECG (ECG shown is similar to patient’s) showed a sinus tachycardia, with no ischaemic changes and apart from the tachycardia, no changes consistent with a pulmonary embolism(PE), or pericarditis.
Lab tests showed a high sensitivity troponin within normal range, normal full blood count and electrolytes and a mildly raised CRP. A D-dimer had been added as the patient’s pain had a pleuritic component and also because we could not rule out a PE using PERC, due to the tachycardia. This was raised at 600ng/mL.
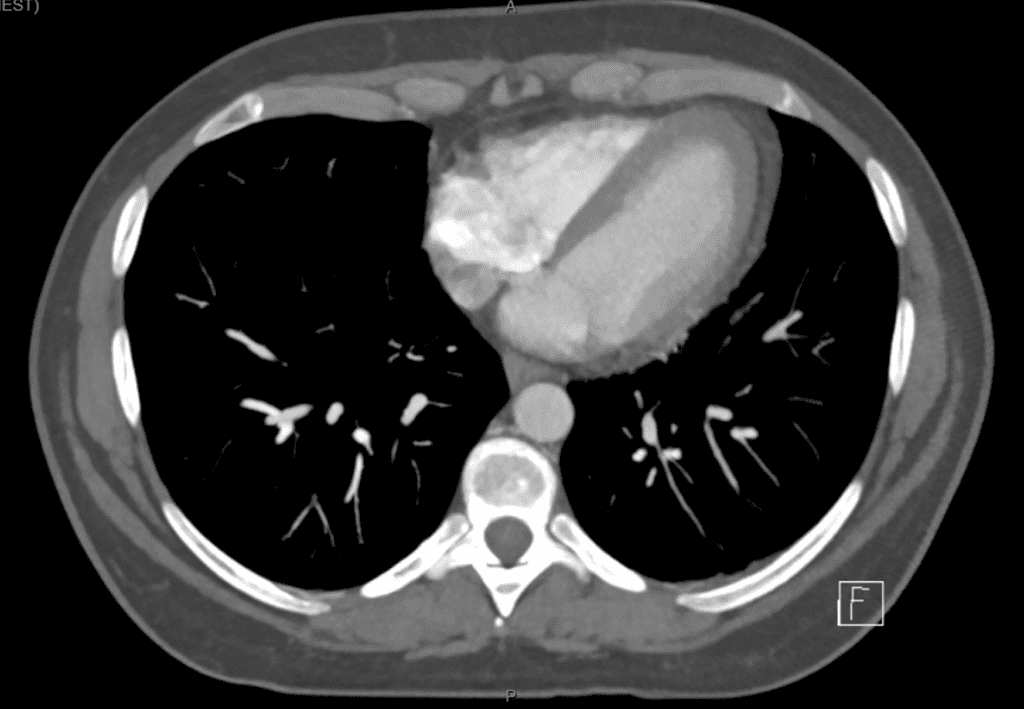
Our suspicion was high enough, that the patient went for a CTPA.

Acute Epicardial Fat Necrosis
Acute epicardial fat necrosis is an inflammatory condition that occurs within the epipericardial fat, leading to encapsulated fat necrosis. It is a benign self limiting disease but may mimic acute coronary syndrome or pulmonary embolism.
There are no risk factors. The cause is not well understood, but thought to be due to either:
- Acute torsion of a vascular pedicle that attaches fatty tissue to the heart, which may lead to necrosis or
- Increased intrathoracic pressure and shearing forces during the cardiac cycle, especially when the adipose tissue has structural anomalies such as lipoma or hamartoma
Clinical Presentation
Patient present with chest pain that is pleuritic in nature and there may also be dyspnea on exertion. The pain recedes over a few days. Examination may be normal and laboratory tests will usually return a normal troponin, although CRP may be elevated. The electrocardiogram is usually non-specific.
Imaging
CT chest allows identification of the lesion which is usually an ovoid-shape soft-tissue mass of adipose tissue density, with a rim. In some cases calcification may develop. MRI can also be used.
Differential Diagnosis
Differential diagnosis includes:
- Lipomas
- Liposarcomas
- Mesotheliomas
- Diaphragmatic hernias
Management
Early treatments included thoracotomy and surgical excision, however the conservative approach is now used, with non-steroidal anti-inflammatory drugs for one to two weeks and a repeat CT in two to three months to check for complete resolution of the lesion. If the diagnosis is uncertain, or there are features of a neoplasm, then thoracotomy and excision is used to make the diagnosis.
Outcome of the Case
The patient was diagnosed with acute epicardial fat necrosis, was commenced on anti-inflammatories and was given advice to stop smoking and reduce alcohol intake and discharged. On follow-up the following day, the patient was feeling better and the chest pain had significantly improved.
References
- Zafar M R et al. Epicardial Fat Necrosis. A Concise Review of the Literature. Cureus 13(2): (February 03, 2021). e13106.







