Introduction
Patients presenting with dizziness comprise about 4% of all emergency department presentations. Our role is to exclude central causes. To be able to do this we an approach that allows us to differentiate central from peripheral causes of dizziness. The diagnosis is far from straightforward and emergency physicians can miss up to one third of strokes in patients presenting with dizziness (1).
The most common causes (up to 43%) of vertigo are benign peripheral disorders. Central causes are usually posterior circulation strokes, comprising 20% of all ischaemic strokes. The posterior circulation comprises the Vertebral, Basilar and the Posterior Cerebral Arteries and their branches. This vertebrobasilar system supplies the brainstem, midbrain, cerebellum, thalamuses and areas of the parietal and occipital cortex and it is the shared neurovascular supply, that results in peripheral and central causes presenting similarly.
The challenge that we face is that up to 20% of patients with a posterior circulations stroke have no signs associated with vertigo or unsteadiness (2,3). Thus, we will not be able to pick up all cases. The usual stroke recognition screening that works for anterior circulation strokes such as FAST (Face, Arm, Speech Test), is far less sensitive when used on the posterior circulation (4). Stroke can also mimic other causes, such as BPPV in 5% of cases and vestibular neuronitis in about 25% of cases (5, 6).
Should we just image every patient with dizziness? CT scans are now readily available in most emergency departments. Performing a quick CT scan gives us false reassurance that we are not missing a stroke. The reality is that CT scans are not sensitive for detecting posterior circulation strokes. At most their sensitivity approaches 50%, but more often that percentage is around 25% (7, 8). We know that twice the number of patients returning to the emergency department with a stroke, had a normal CT brain, before being discharged on their previous presentation.
Diffusion weighted MRI is considered the gold standard for making the diagnosis. It is not readily available, nor is it readily accessible. Further, it may miss 20% of small ischaemic strokes within the first 48 hours of symptom onset (7).
Peripheral Causes Dizziness
- Benign Paroxysmal Positional Vertigo (BPPV)
- An inner ear disorder characterised by brief, rapid onset of repeated episodes of vertigo on head movement. It is associated with nausea, vomiting and unsteadiness. The cause is usually an otolith moving into the semicircular canals. Diagnosis is made by history and performing the Dix-Hallpike and Pagnini-McClure manoeuvres.
- Dix-Hallpike (tests posterior semicircular canals)
- Pagnini-McClure (often called the supine head roll) tests lateral semicircular canals
- An inner ear disorder characterised by brief, rapid onset of repeated episodes of vertigo on head movement. It is associated with nausea, vomiting and unsteadiness. The cause is usually an otolith moving into the semicircular canals. Diagnosis is made by history and performing the Dix-Hallpike and Pagnini-McClure manoeuvres.
- Vestibular Neuronitis
- A benign, self-limiting condition resulting from inflammation of the vestibular portion of Cranial Nerve 8. Patients present with vertigo, nausea and gait imbalance, which can last for several weeks. It is usually caused by a viral infection and is diagnosed clinically. Patients may present similarly in labyrinthitis, but there is no hearing loss here.
- Labyrinthitis
- This is caused by an inflammation of the labyrinth of the inner ear, due to a bacterial or viral infection, or systemic autoimmune disease. Patients present with vertigo, nausea, vomiting and tinnitus. There may also be hearing loss. Patients may be left with balance impairment, or hearing problems.
- Meniere’s Disease
- This can present similarly to labyrinthitis, however episodes are intermittent. It is caused by endolymph build-up in the labyrinth. Patients present with vertigo, tinnitus, hearing loss and a feeling of aural fullness. Attacks are intermittent, however in some cases they are severe causing ‘drop attacks’.
- Vestibular Migraine
- It can be associated with a headache, but does not need to be. Patients present with vertigo, nausea and vomiting and imbalance. The diagnosis is clinical and involves an association between a history of migraines and episodic vertigo, which can last from minutes to days.
History and Examination
History and examination is considered the best way to make a diagnosis. In most cases the diagnosis can be made by taking a good history. Diagnositic approaches have also been proposed to improve our ability to diagnose stroke.
These diagnostic approaches include (more on these below):
- The HINTS (Head Impulse, Nystagmus, Test of Skew)
- STANDING (SponTAneous, Nystagmus, Direction, head Impulse test, standiNG
- ABCD2 (Age, Blood pressure, Clinical features, Duration, Diabetes)
History
Patients often present with a complaint of dizziness. They may not describe vertigo, but call it dizziness. This can have several meanings for the patient including, lightheadedness, imbalance, vertigo or weakness. Trying to understand the character of the dizziness, by asking the patient to explain what they mean by ‘dizzy’ is associated with misdiagnosis 8,9).
It is more important to ascertain some of the following:
When did this start and has it occurred before?
-
- Prolonged causes of dizziness or vertigo include:
- Central Causes ie posterior circulation stroke
- Vestibular neuronitis
- Is it episodic or continuous?
- Does it recur and when it does how long does it last? Recurrent episodes may be due to a TIA, however frequent recurrence is usually of peripheral causes such as:
- Meniere’s Disease
- BPPV
- Vestibular Migraine
- Continuous points to a central cause, however having vertigo for a very long time is unusual as even in stroke, adaptive mechanism may dampen the vertigo.
- Does it recur and when it does how long does it last? Recurrent episodes may be due to a TIA, however frequent recurrence is usually of peripheral causes such as:
- Prolonged causes of dizziness or vertigo include:
Are there triggers or is it spontaneous?
-
-
- Triggers such as head movement indicate a peripheral cause such as BPPV
-
Is there a history of migraines and is there any relationship to the symptoms?
-
-
- Can this be a vestibular migraine? We need to remember that in some cases there is no relationship between the headache and the symptoms, which make it difficult to diagnose.
- Vestibular -evokes myogenic potentials(VEMP) can be used to differentiate migraine from Meniere’s disease or BPPV.
-
Is there hearing loss and does the patient have tinnitus?
-
-
- This indicates a diagnosis Meniere’s Disease or Labyrinthitis
-
Is the patient able to get out of bed and walk around, even if holding onto things?
-
-
- Patients with central causes have truncal ataxia in over 60% of cases. In many cases they cannot get out of bed and cannot mobilise (although not always)
- Patients with peripheral causes of dizziness, do not have truncal ataxia and are usually able to mobilise, even if they have to support themselves by holding onto furniture.
-
Have the patient had a recent viral or other illness
-
-
- This history may allow us to diagnose vestibular neuronitis or labyrinthitis.
- The two conditions present similarly, however there is hearing loss in labyrinthitis.
-
Prediction Tools
There are three main clinical tools evaluated for predicting central causes of vertigo. They are:
- ABCD2
- HINTS
- STANDING
ABCD2 Score
This is a clinical prediction rule for assessing stroke risk following a transient ischaemic attack (10).
It is made up of 5 clinical features that have points associated with them:
A (Age)
- If a patient is > 60 years old (1 point)
B (Blood Pressure)
- > 140/90 (either SBP>140 or DBP >90) (1 point)
C (Clinical features)
- Unilateral weakness (2 points)
- Speech disturbance without weakness (1 point)
- Any other symptoms (0 points)
D (Duration of Symptoms)
- < 10 minutes (0 points)
- 10-59 minutes (1 point)
- > 60 minutes (2 points)
D(Diabetes) (1 point)
0-3 points: low risk
4-5 points: moderate risk
6-7 points: high risk
In a retrospective observational study (13) it was found, as might be expected, that those patients with a low score presenting with dizziness had a lower risk of a cerebrovascular diagnosis. However this score can fail to predict half of the cases of stroke (14).
HINTS EXAMINATION
In order to perform the HINTS test, nystagmus must be present. HINTS comprises 3 parts:
- Head Impulse Test (HIT)
- The patient is asked to continue looking straight ahead as the head is rotated from side to side by the examiner. The eyes must remain stationary and fixate on the central target. With an acute vestibular lesion, the input from the opposite side is unopposed and when the head is moved towards the affected side, the eyes will move towards that side and then there will be a corrective saccade. A positive test and indicates peripheral pathology.
- Nystagmus
- This is the rhythmic involuntary eye movement that occurs when the patient is asked to look laterally. The direction of the nystagmus is named after the fast component. In the normal patient the nystagmus is limited to a few beats and decays with fixation and is purely horizontal. Anything other than unidirectional horizontal nystagmus is considered abnormal. Abnormal nystagmus includes:
- Vertical nystagmus
- Bidirectional nystagmus
- Rotational nystagmus
- See-saw nystagmus
- Test of Skew
- This involved covering the eye for several seconds and then uncovering it rapidly. The eye deviates when covered and re-aligns vertically to correct when uncovered. This movement may indicate a central cause of nystagmus.
- This is the rhythmic involuntary eye movement that occurs when the patient is asked to look laterally. The direction of the nystagmus is named after the fast component. In the normal patient the nystagmus is limited to a few beats and decays with fixation and is purely horizontal. Anything other than unidirectional horizontal nystagmus is considered abnormal. Abnormal nystagmus includes:
The HINTS examination has a very high sensitivity (97%) and specificity (95%), when performed by trained specialists. The sensitivity ans specificity has been found to drop when performed by emergency physicians to 83% and 44% respectively (14)
STANDING ALGORITHM
Vanni et al (12) proposed a structured diagnostic approach:
- Assess for Nystagmus (with and without Frenzel glasses)
- If there is no spontaneous nystagmus in the supine position, look for positional nystagmus which will confirm a diagnosis of BPPV, using:
- Dix-Hallpike to assess for posterior semicircular canal involvement and
- Pagnini-McClure Manoeuvre: where the patient rolls their head 90 degrees to each side, assessing the lateral semicircular canals.
- If nystagmus was already present in the supine position and it was persistent, the position was assessed. Assess the Nystagmus. It is a central cause if it is:
- Vertical or
- Multidirectional
- If Spontaneous Nystagmus is present and unilateral, test the vestibulo-ocular reflex with HIT.
- A positive HIT identifies peripheral vestibulopathy
- A negative HIT bilaterally indicates a central cause.
- If patients had no nystagmus, gait was evaluated. If the patient was unable to stand without assistance, a central cause was considered.
- If there is no spontaneous nystagmus in the supine position, look for positional nystagmus which will confirm a diagnosis of BPPV, using:
In this study the sensitivity was found to be 100%, with wide confidence intervals. Of 72.3-100% and a high specificity of 94.3% (90.7-94.3). Repeated studies have found sim ilar good sensitivity and specificity (13).
Nystagmus us a very important part of making the diagnosis in the patient with dizziness/vertigo. Peripheral causes of dizziness will have associated unilateral nystagmus. Visual fixation is the enemy of the examiner as it results in resolution of nystagmus. For this reason Frenzel lenses have been used before. These allow the eyes to be magnified and they also restrict the patient from fixation. These lenses are not readily available, so an alternative is to use the ‘penlight cover test’.

To perform the penlight cover test, the examiner covers one of the patient’s eyes and then shines the torch light into the other eye. This momentarily stops the patient from being able to fixate on any object and any masked nystagmus may be revealed.
Examination
How accurate is the neurological Examination?
In a meta-analysis (16), it was found that some examinations are difficult to elicit. It appears that in many instances the sensitivity is low.
| Examination | Sensitivity (%) | Specificity (%) |
| Dysmetria | 24.6 | 97.8 |
| Limb Weakness/Hemiparesis | 11.4 | 98.5 |
| Spontaneous Nystagmus | 52.3 | 42 |
| Truncal / Gait Ataxia | 69.7 | 83.7 |
| Test of Skew | 23.4 | 97.6 |
| HIT | 76.8 | 89.1 |
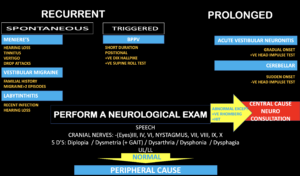
An Approach to the Patient with dizziness ( See figure below)
- Decide if this is recurrent or prolonged
- If recurrent, is it
- Spontaneous: Causes will include:
- Meniere’s Disease
- Vestibular Migraine
- Labyrinthitis
- Triggered, especially on head movement: The cause will be BPPV
- Spontaneous: Causes will include:
- If recurrent, is it
- Perform a Neurological Examination: Especially looking for:
- Cranial Nerve Signs
- Nystagmus
- Diplopia
- Dysphagia
- Perform HIT and Test of Skew
- Speech
- Dysphonia
- Cerebellar Signs
- Dysmetria
- Truncal Ataxia
- Weakness: Upper and Lower Limb Weakness
- Cranial Nerve Signs
REFERENCES
- Kerber KA et al. Stroke among patients with dizziness, vertigo and imbalance in the emergency department: a population-based study. Stroke 2006;37(10:2484-2487
- Tamutzer AA et al. Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. Can Med Assoc. J. 2011;183(9):571-592.
- Venhovens J et al. Acute vestibular syndrome: a critical review and diagnostic algorithm concerning the clinical differentiation of peripheral versus central aetiologies in the emergency department. J Neurol. 2016; 263(11):2151-2157.
- Gulli G, Markus HS. The use of FAST and ABCD2 scores in posterior circulation, compared with anterior circulation, stroke and transient ischemic attack. J Neurol Neurosurg Psychiatry 2012;83:228-9.
- Tamutzer AA et al. ED misdiagnosis of cerebrovascular events in the era of modern imaging: a meta analysis. Neurology. 2017;88(15):1468-1477
- Blum CA et al. Transient ischaemic attacks presenting with dizziness or vertigo. Neurol Clin 2015;33(5):629-642.
- Shah VP et al. Diagnostic accuracy of neuroimaging in emergency department patients with acute vertigo or dizziness: a systematic review and meta-analysis for the guidelines for reasonable and appropriate care in the emergency department. Acad Emerg Med. 2022;97(5):507-520.
- Chalela JA et al. Magnetic resonance imaging and computed tomography in emergency assessmenmt of patients with a suspected acute stroke: a prospective comparison. Lancet. 2007;369(9558):293-298.
- Voetsch B et al. Acute dizziness, vertigo and unsteadiness. Neurol Clin. 2021;39(2):373-385.
- Stanton V et al Over reliance on symptom quality in diagnosis dizziness: results of a multicenter survey of emergency physicians. Mayo Clin Proc. 2007;82(11):1319-1328.
- Johnson SC et al. Validation and refinement of scores to predict very early stroke tisk after transient ischaemic attacks. Lancet 2007;369:283-292.
- Vanni S et al. STANDING, a four-step bedside algorithm for differential diagnosis of acute vertigo in the emergency department. Acta Otorhinolaryng Ital 2014;34:419-426.
- Navi B et al. Application of the ABCD2 Score to identify Cerebrovascular Causes of Dizziness in the E,mergency Department. Stroke. 2012;43:1484-1489.
- Gerlier C et al. Differentiating central from peripheral causes of acute vertigo in an emergency setting with HINTS, STANDING and ABCD2 tests: A diagnositic Cohort Study. Acad Emerg Med 2021;28:1368-1378
- Ohle R et al. Can emergency physicians accurately rule out a central cause of vertigo using HINTS examination? A systematic review and meta analysis. Acad Emerg Med 2020;27(9):887-896.
- Vanni S et al. Can emergency physicians accurately and reliably assess acute vertigo in the emergency department? Emerg Med Australas. 2015;27(2):126-131.







