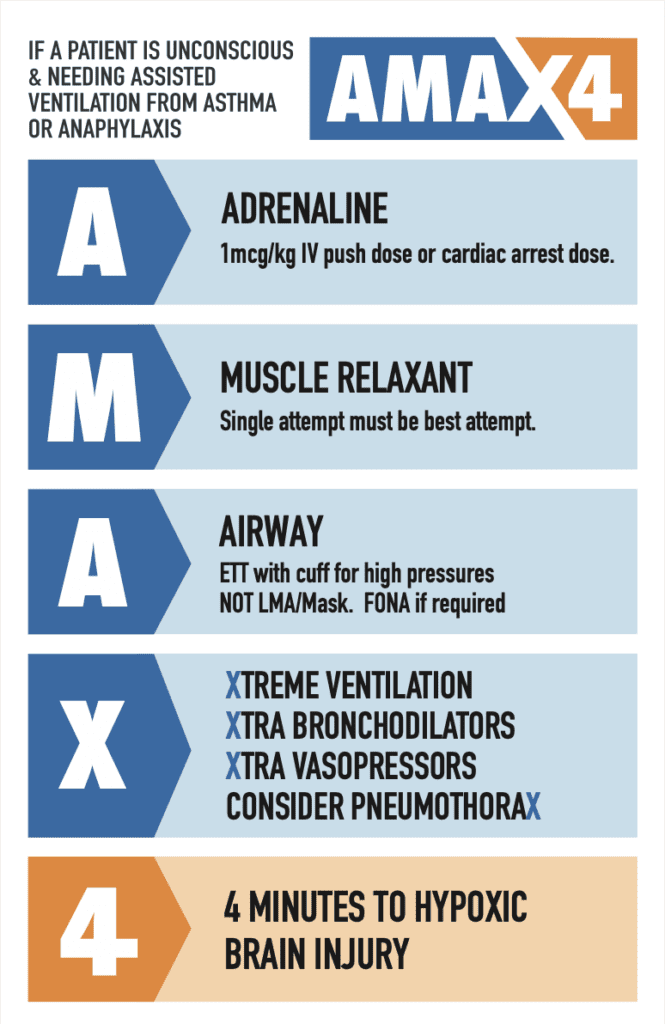
I recently had the pleasure of speaking to Dr Ben McKenzie, Emergency Physician and researcher into anaphylaxis. Ben has developed the AMAX 4 algorithm. The AMAX4 algorithm gives a cognitive aid to managing anaphylaxis – whether by using the mnemomic, or understanding there is “a max of 4 minutes” to achieve brain oxygenation through iv adrenaline and intubation in the unconscious patient. I have previously written about AMAX4.
Below is an interview with Ben about his work and AMAX4.
Watch the full interview is at emmastery.com.
Pearls in Anaphylaxis
- There are 2 opportunities in Emergency Medicine to save someone’s life from anaphylaxis:
- The first is during resuscitation: HYPOXIC BRAIN INJURY OCCURS IN 4 MINUTES
- The second is on discharge, by advising the patient that the core of treatment is allergen avoidance and giving them proper discharge support.
- Anaphylaxis is a type I hypersensitivity reaction. It has a trigger which leads to a rapid onset, peak, and resolution that can occur within 4 hours.
- It is not viral urticaria, ACEI induced or idiopathic angioedema, idiopathic urticaria or vocal cord dysfunction
- It is the shortest life threatening multi-organ disease in medicine
- Approximately 98% of anaphylaxis lasts less than 4 hours.
- The median length of stay in ICU for adults and children is less than 24 hours.
- 50% of adult ICU admissions in Australia have already improved by the time they are physically admitted and do not require organ support.
- 25% are intubated.
- Any allergen can cause compromise of airway (oropharyngeal or laryngeal), bronchospasm or cardiovascular system. They may occur simultaneously.
- Insect allergy (jack jumper, fire ants, bees, wasps , ticks) is almost always hypotension and airway symptoms.
- Food allergy is most frequently bronchospasm and airway symptoms (eg cows milk, tree nuts, peanuts, sesame, seafood). All deaths occur from respiratory arrest – almost exclusively from bronchospasm. Food allergies are the predominant trigger in ED in both children and adults.
- Food anaphylaxis onset is usually less than 30 minutes but onset can be variably delayed. From a patient having compensated vital signs to cardiorespiratory arrest can be as little as 5 minutes, even in food allergy.
- Drug allergy is a mixture of hypotension and bronchospasm and heavily influenced by underlying medical problems, drugs and other concurrent treatments like propofol/anaesthesia. 60-70% of deaths involve bronchospasm.
- Onset of symptoms is less than 5 minutes for IV drugs/contrast and often immediate.
- The focus of anaphylaxis treatment is providing oxygen and blood pressure to avoid brain injury and death from hypoxia and hypotension. We cannot predict, when a reaction has started and treatment has commenced, who is at risk of deterioration and will require intubation and intensive cardiovascular support – the disease must be respected despite the vast majority responding to simple treatment – they must be triaged to a resuscitation area if symptoms are present. Pre-arrest symptoms and signs include saying “I can’t breath”, “I’m going to die”, incontinence, hypoxia on oxygen, agitation. NIV +/- ketamine may help if there is time to gain control before unconsciousness.
- Adrenaline, a non selective adrenoreceptor agonist is the mainstay of treatment in anaphylaxis. It provides airway, breathing and circulation end organ support. It is uncertain whether it shortens anaphylaxis in vivo (probably doesn’t). Other bronchodilators and blood pressure support should be used in refractory or severe cases.
- IM adrenaline is benign. Give when you are worried about the patient. Airway, breathing and circulation symptoms are hard indications.

- IM adrenaline takes 5 minutes to reach peak levels before falling and then slowly rising for a second peak that lasts approximately one hour (or longer). This is why IM adrenaline is a 5 minutely drug. This is approximately 5-8mcg/min over an hour for an adult 500mcg dose although in two peaks and the 5 minute time point equivalent IV rate is much higher.
- Thigh is best for distribution, as upper limb results in lower levels in the bloodstream. Ensure the needle is long enough to traverse subcutaneous tissue.
- In ED 90% need only one dose of IM adrenaline. 7.7% need more than one dose. Only 2.2% needed 3 doses or more.
- Mortality dramatically jumps if symptoms are refractory despite 2 doses of IM adrenaline – this a red flag.
- IV adrenaline infusion is indicated if refractory to 2 doses of IM adrenaline (10 minute mark of treatment). Awake patients: Start low and titrate up to ABC symptoms. Unconscious patients – start high (0.5mcg/kg/min and titrate down/up).
- IV adrenaline bolus 1mcg/kg every 2-3 minutes is indicated in unconscious patients where 5 minutes to IM adrenaline is far too long to wait for an effect (and poor absorption) and an IV infusion takes 10 minutes to prepare. This is one tenth of the cardiac arrest dose. Remember hypoxic brain injury occurs in 4 minutes,
- Mediators may still be present or increasing and symptoms dramatically increase while adrenaline is wearing off – Call these rebound symptoms and better still describe what happened to your colleagues rather than calling them biphasic.
- Symptom recurrence is rarely significant after adrenaline has worn off and the patient is asymptomatic – so called biphasic reactions – controversial and overstated.
- Catastrophic bronchospasm requires immediate endotracheal intubation to be able to ventilate obstructed lower airways using high PIPs. Subsequent obstructive ventilation techniques are essential to achieve successful oxygenation and avoid barotrauma – small tidal volumes, high pressure/high inspiratory flow during inspiration, long expiratory time, 100% oxygen, consider ECMO.
- On discharge
- ALLERGEN AVOIDANCE: most people who die from food/insect allergens have usually only had mild reactions before and most have seen a doctor like you
- Urticaria and mouth itchiness triggered by cashews in a school aged asthmatic is extremely significant despite not meeting anaphylaxis criteria – they are likely to be at risk of death on re-exposure – an allergist will risk stratify
- Epipen and action plan if at risk of re-exposure
- Referral to allergist for confirmation, risk stratification and life long support.
- Insect allergens for venom desensitisation program
- Food allergen: Asthma must be controlled. Education that shortness of breath/asthma symptoms is the most life threatening symptom – Calling the ambulance is as important as the epipen.
- Steroids on discharge?: anaphylaxis is usually over before steroids work by upregulating adrenoreceptors although they are absolutely indicated at the onset of critical bronchospasm/airway oedema as the duration of the reaction is unknown at that point
- ALLERGEN AVOIDANCE: most people who die from food/insect allergens have usually only had mild reactions before and most have seen a doctor like you
I invite you to go to Ben’s site and watch the one hour AMAX4 Lecture. it is broken up into 6 x 10 minute mini lectures that are easy to watch, thought provoking and will hopefully help you make adjustments to your practice.







