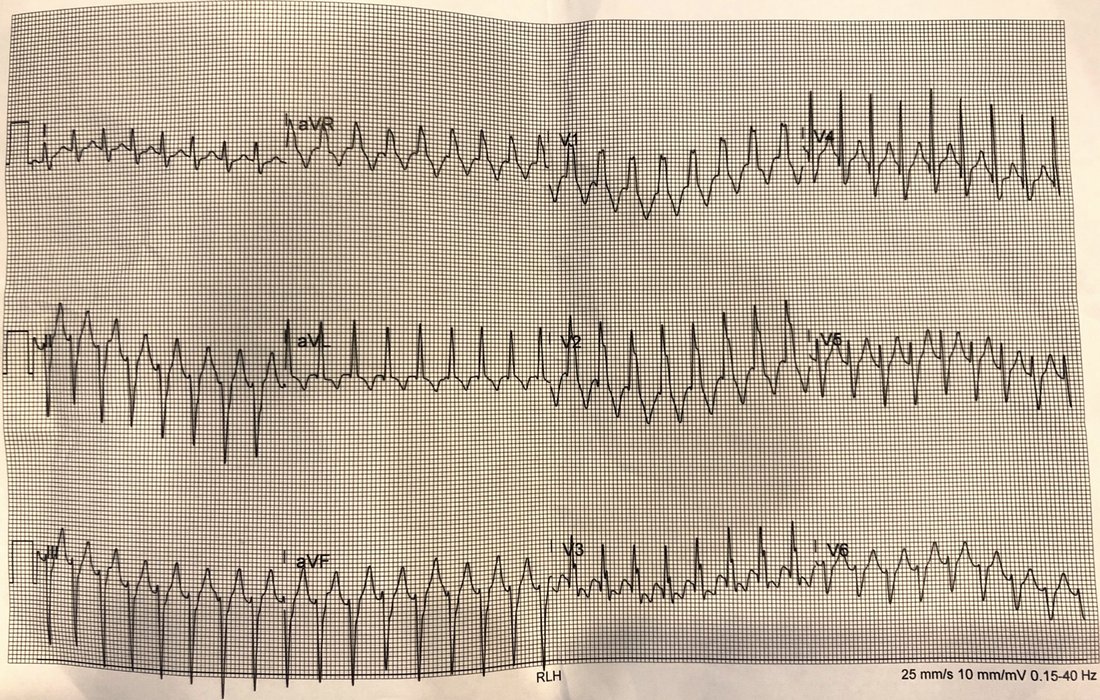
What does the ECG show?
What is the diagnosis? Is it VT or SVT?
Let me know what you think. Answers (plus more history) in next weeks blog, plus a simplified method of arrhythmia diagnosis.
My response to the ECG without any history was:
It is real ie not a mimic.
It is regular
The rate is faster than 120bpm, so we can consider VT. It is a little too fast perhaps at about 198, but can still be VT
The QRS width is just wider than 120ms ie., 124ms. It is a little borderline, but favours VT
There is no concordance
There is a dominant R wave in avR which favours VT
There is no AV dissociation that I can see
The morphology is RBBB with an Rsr which favours VT, also the R/S in V6 is <1 ( ie the QRS is entirely negative in V6)which favours VT.
Rx Cardioversion is probably safest. If not haemodynamically unstable, you could give adenosine. If VT, nothing would happen, if SVT will cause an AV block and may revert. (Adenosine is also safe to give as this is a regular rhythm,)
I would add to this that there is a borderline left axis deviation
The rest of the story….
The history at presentation was that the patient developed palpitations whilst running. There was a long history of SVT, for which he had an ablation several years previously.
The cardiac history was more significant in that the patient had had endocarditis some 14 years previously. As a consequence there had been an aortic and mitral valve repair. Several years after this, he had an aortic root replacement.
The patient had attempted valsalva manoeuvres, with no success.
He was haemodynamically stable.
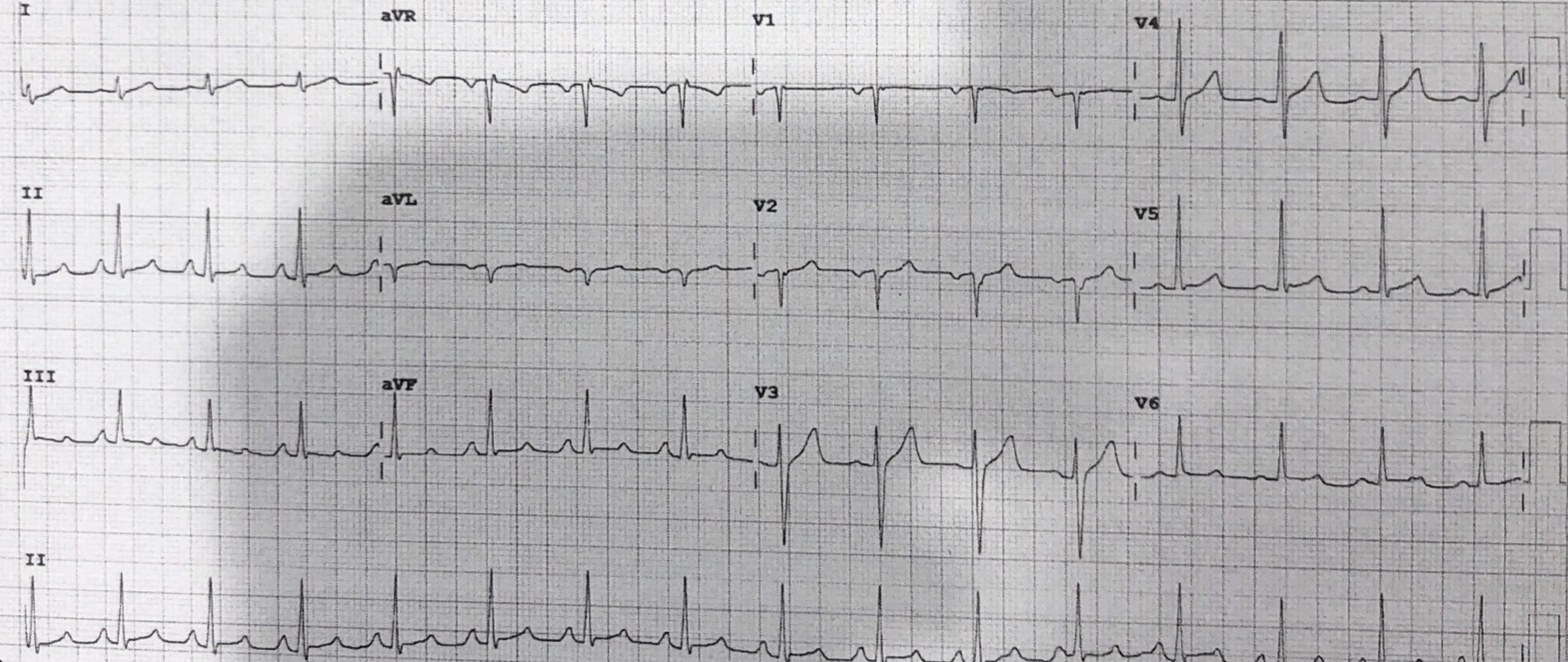
The patient was treated with Magnesium 5mmol, 500ml of IV fluid stat and Metoprolol and reverted to sinus rhythm.
His ECG was shown below. It shows atrial enlargement with some inverted p waves in V2.
Comments
What would you have done?








An interesting one.
But why was Metoprolol used instead of Adenosine ?
why the magnesium was given?