AMAX4 is a treatment algorithm for anaphylaxis and asthma resuscitation.
It was developed by emergency physician Ben McKenzie following the tragic death of his 15 yo son Max, from anaphylaxis induced bronchospasm. Max was awake and talking, when first receiving emergency care, however despite care, he deteriorated to a hypoxic cardiac arrest, with no airway secured for significant amount of time. He sustained an unsurvivable hypoxic brain injury.
Max was a happy, loving and talented young man and his death is a tragedy. Ben has made it a mission to develop knowledge and an approach to anaphylaxis, so this doesn’t happen to anyone else.
Firstly, I invite you to go to Ben’s site and watch the one hour AMAX4 Lecture. it is broken up into 6 x 10 minute mini lectures that are easy to watch, thought provoking and will hopefully help you make adjustments to your practice.
DEFINITION of ANAPHYLAXIS
As per the World Allergy Organisation, Anaphylaxis can have one of two definitions.
Definition 1
Acute onset of an illness (minutes to several hours) with simultaneous involvement of the skin, mucosal tissue, or both (eg, generalized hives, pruritus or flushing, swollen lips-tongue-uvula)
AND AT LEAST ONE OF THE FOLLOWING:
- Respiratory compromise (eg, dyspnea, wheeze-bronchospasm, stridor, reduced PEF, hypoxemia)
- Reduced BP or associated symptoms of end-organ dysfunction (eg, hypotonia [collapse], syncope, incontinence)
- Severe gastrointestinal symptoms (eg, severe crampy abdominal pain, repetitive vomiting), especially after exposure to non-food allergens
Definition 2
Acute onset of hypotension or bronchospasm or laryngeal involvement after exposure to a known or highly probable allergen for that patient (minutes to several hours), even in the absence of typical skin involvement.
THE BASICS
- When a cardiac arrest occurs due to cardiac aetiology, the patient, in most cases, will have good oxygen saturations. In a hypoxic arrest, the opposite is true. The patient will be hypoxic with de-oxygenated blood.
- Why do we apply the same resuscitation algorithm to both?
- Performing CPR on a hypoxic patient, simply circulates deoxygenated blood to the brain.
- The brain has no oxygen stores. Hypoxic brain injury occurs in 4 minutes. If we delay oxygenation, the patient will die, or have severe neurological impairement.
- Airway in Anaphylaxis means rapid intubation with a cuffed endotracheal tube. No Bag Valve Mask and No Laryngeal airway will be able to seal the airway against the large pressures that are generated, in the same way that a cuffed endotracheal tube can.
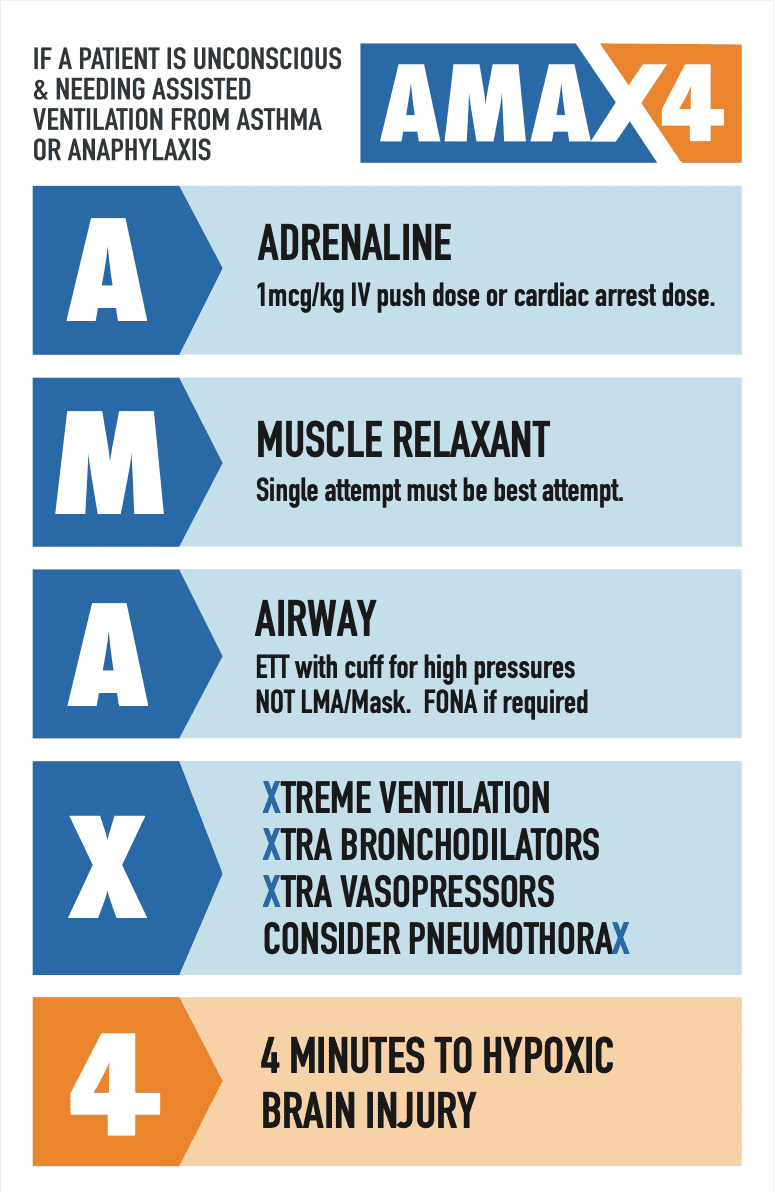
THE ALGORITHM

THE ALGORITHM BROKEN DOWN
Start with the end in mind

Hypoxic brain injury occurs within 4 minutes. When a patient arrests due to a respiratory cause such as bronchospasm, the blood is severely deoxygenated leading to a respiratory arrest and consequently a cardiac arrest. The best CPR will simply send deoxygenated blood to the brain. The brain has no oxygen reserves. Hypoxic brain injury will occur early…after 4 minutes.
Intramuscular Adrenaline takes too long to work. Absorption takes longer than the 4 minutes for brain injury. Intravenous Adrenaline works quickly and can be titrated. In most adult patients we can give 70-100 mcg IV. If the patient has already arrested, consider the full cardiac dose. Push Adrenaline every 30 seconds to 10 minutes at a dose of 1 mcg/kg IV
How to draw up IV push adrenaline
- 1 mL of 1:1000 Adrenaline.
- Draw this 1mL into a 10mL syringe, then make up the other 9mL with normal saline.
- The concentration is then 100 mcg/mL
- For younger patients draw up 1mL of the 100 mcg/ml concentration into a 10ml syringe, diluting with 9mL of normal saline to make a full 10mL
- The concentration is now 10 mcg/mL

If the patient is fully arrested, then cold intubation is fine. If there is any chance of airway reflexes being intact, then paralyse the patient. The first intubation attempt should be the best attempt, so we aim for the best conditions by paralysing and we always get the most experienced operator to perform the procedure. Intubation of this patient must be performed as this patient will not improve.
Use a Video Laryngoscope and intubate with a cuffed endotracheal tube(ett).
Why an endotracheal tube?
- Airway pressures will be high; up to 100cm H20. A cuffed tube is needed to handle these.
- The risk of aspiration is high. The initial bagging that occurs, is done against a possible swollen and constricted airway and oxygen will pass through the path of least resistance ie., into the stomach
NO BVM: Stomach will be ventilated: path of least resistance
NO Supraglottic Airway: Cannot handle the pressures
May need a Surgical Airway: Remember 4 minutes is what we have. One good attempt at intubation, is all there is time for. If this is not possible, then consider a surgical airway.
Post intubation use BVM to ventilate via the ett, rather than immediately connecting to the ventilator
Give Bronchodilators as needed.
Add more vasopressors as needed ie., NorAdrenaline, Vasopressin etc.
The rates of Pneumothorax are high in the arrested bronchospasm patient where CPR has been performed. The chest may need to be decompressed.
‘Just a Routine Resuscitation’
‘This video was produced by Tamara and Ben McKenzie with critical care clinicians demonstrating the use of the AMAX4 algorithm in the treatment of hypoxic anaphylaxis and asthma. The first half of this video is Tamara and Ben talking about what happens in the resuscitation. Ben arrives in the resuscitation at the hospital he is working in and has to take over the resuscitation of his own son. …. No-one should ever have to do that.
The second half shows a simulation of how it should be done.
This is an emotional video and it should be. We can never forget that the patient we are treating is someones son or daughter, mother or father, sister or brother. Please watch.
Just A Routine Operation
The video below is of a very famous airway case. Mrs Elaine Bromiley, attended hospital for an elective routine nasal procedure. She was a well 37 years old, mother-of-two. After induction of anaesthesia there were difficulties in securing her airway. The patient was hypoxic for a prolonged period of time. It was not recognised that this was a ‘Can’t Intubate, Can’t Ventilate’ scenario and there were continued attempts to intubate.
We need to remember that the decision to perform a surgical airway must be made early. 4 minutes is all it takes.







