A 68 yo patient presents with two hours of central chest pain and dyspnoea and some diaphoresis. Past medical history is hypertension.
Vitals are HR is 72, BP 134/60, Sats 98% on room air GCS is 15.
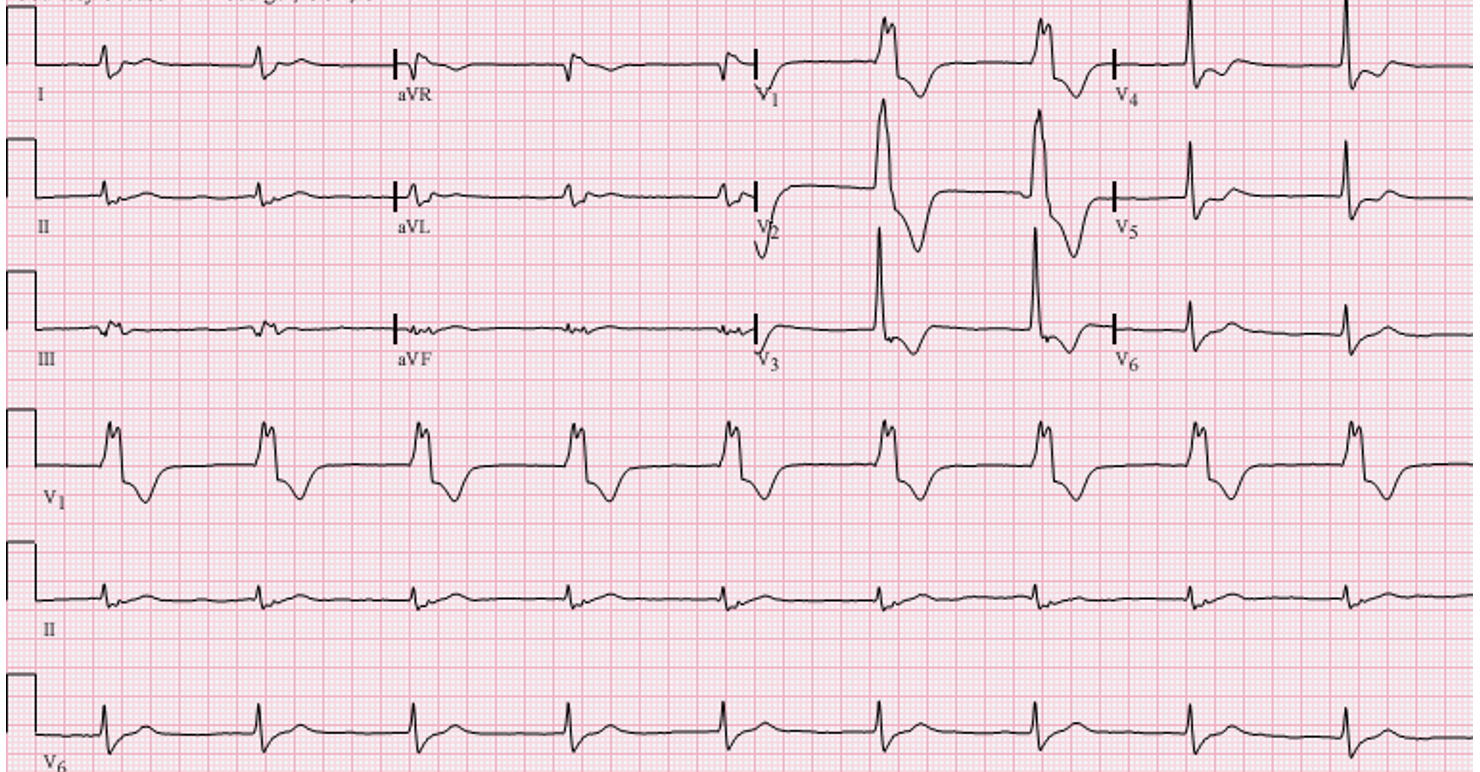
An ECG is done which shows and anterior STEMI. The patient continues to be haemodynamically stable.
You have no cath lab in your hospital, so it is decided to thrombolyse the patient in the emergency department.
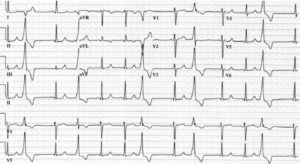
A short time following completion of the thrombolytic, the monitor alarms and you see several wide complexes. The patient is haemodynamically stable. An ECG had captured this and is shown below. What does it show?
Following completion of this case, we should be able to answer the following questions:
- What is a reperfusion arrhythmia/escape rhythm?
- What types of reperfusion arrhythmias are there?
- How to identify AIVR?
- How to differentiate AIVR from VT?
- What is the safest treatment for escape rhythms?
Ind pacing and electrophys jrnl. 2010. 357-71
These are premature ventricular complexes (PVC). PVCs may represent an escape pacemaker. As with all escape rhythms the use of antiarrhythmics, such as beta blockers, may suppress this escape pacemaker resulting in severe bradycardia and asystole. Although there is some concern that left untreated, PVCs may deteriorate into ventricular fibrillation, this is not always seen and in most cases they simply spontaneously resolve.
…….These PVCs terminate soon after.
Approximately 20 minutes later you are called to the bedside as the patient has developed a wide complex rhythm. The patient is haemodynamically stable. An ECG is shown below. What is this rhythm and how should we manage this?
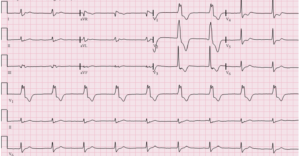
This is Accelerated Idioventricular Rhythm (AIVR).
AIVR
AIVR is a wide complex rhythm, consisting of three or more monomorphic ventricular beats, with a rate of 40-110 bpm. There may be AV dissociation, when the sinus rate slows and the ectopic focus appears, or when the ectopic focus accelerates above the sinus rate. The ectopic focus originates from the His-Purkinje system.
It usually starts gradually, following a long premature ventricular beat or with a slowing of the sinus rate. It may terminate gradually or abruptly, as the sinus rate increases.
Atrial and ventricular beats may have similar rates, ie., isorhythmic AV dissociation, which can result in capture and fusion beats (see below). Isorhythmic AV dissociation, should not be confused with complete heart block, where the atrial rate is faster than the ventricular rate.
AIVR is the most common arrhythmia seen in reperfusion and occurs in up to 20% of patients with acute myocardial ischaemia and infarction. It is considered a reperfusion arrhythmia, however it is neither sensitive nor specific for reperfusion, as it also occurs in patients where reperfusion has not occurred.
AIVR can also occur in the athlete, where there is no structural heart disease, but it is the result of an increase in vagal tone. It can also occur in myocarditis, cocaine and digoxin toxicity.
AIVR is an escape rhythm which usually self-resolves and is thus considered benign. In the asymptomatic patient, it should be left untreated, as there is no evidence that it leads to ventricular fibrillation(VF). Blocking this escape rhythm may lead to bradycardia and asystole.
If the rhythm doesn’t self terminate or if it leads to haemodynamic instability or ischaemia, then temporary pacing can be used.
…….A short time later the AIVR self terminates.
Within the next hour the registrar calls you to the resus cubicle as the the patient has has had a short run of wide complex tachycardia. It has been captured on ECG. What does the ECG show? How should we manage this episode?
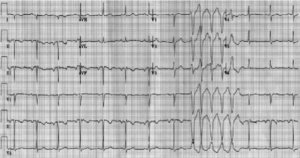
This is non-sustained Ventricular tachycardia (VT). Ventricular arrhythmias occur in several phases. the first is within the first 72 hours post AMI and it affects 6% of patients. The significance of these early sustained ventricular arrhythmias, on mortality, is uncertain.
VT can be differentiated from AIVR, by its rate. VT will have a rate greater than 120bpm, whereas AIVR will have a ventricular rate of 40-110 bpm.
VT can be non-sustained or sustained. Non-sustained VT as seen in this patient’s ECG is defined as 3 or more complexes lasting less than 30 seconds. A single episode is of little concern, however, multiple episodes put patients at risk of becoming haemodynamically compromised. Treatment is aimed at correcting electrolytes, (K > 4.5mmol/L and Mg > 2mmol/L) or treating the ischaemia.
Sustained ventricular tachycardia can be monomorphic, which is usually related to myocardial scar tissue, or polymorphic, which is ischaemic in origin and associated with a mortality of 20%. VT can deteriorate into VF.
If there is haemodynamic instability, VT requires immediate cardioversion (synchronisd in monomorphic VT and unsynchronised in polymorphic VT) and correction of electrolytes.
If the arrhythmia continues to occur, then overdrive pacing can be used to terminate it.
VF may also occur purely due to ischaemia. The greatest incidence of VF, is in the first hour following infarction.
Reperfusion Arrhythmias
The above are examples of reperfusion arrhythmias. Reperfusion arrhythmias occur early (usually in the first hour) following the restoration of coronary blood flow. They are believed to be caused by an excess of intracellular calcium, although this is not completely understood. The earlier and more rapid the reperfusion, the greater the chance of reperfusion arrhythmias occurring. We need to remember that ischaemia may produce arrhythmias which are very similar.
Abnormalities, such as conduction disturbances, which include heart blocks can also occur.
Most reperfusion arrhythmias will resolve spontaneously. Treatment is used when haemodynamic instability occurs.
Treatment Strategies
AIVR
This will usually self-resolve. Do not treat with antiarrhythmics due to risk of blocking the escape rhythm and causing bradycardia or asystole. Temporary Pacing can be used in patients where this is sustained, or results in haemodynamic compromise.
Premature Ventricular Complexes
Do not use antiarrhythmics as they may suppress the escape pacemaker.
VT
Multiple runs of non-sustained VT are associated with increased risk of haemodynamic compromise. Treatment is aimed at correcting electrolytes, or treating the ischaemia.
Sustained VT, may be either monomorphic or polymorphic. If there is haemodynamic instability, it requires cardioversion and correction of electrolytes.
If the arrhythmia continues to occur then use overdrive pacing to terminate it.
Antiarrhythmic Medications
The use of antiarrhythmics in the early period post infarction is not well studied.
Beta Blockers
Beta blockers lower automaticity and are effective for recurrent VT or VF. They should not be given to escape rhythms and care taken to not be given in significant bradycardias or right coronary ischaemia.
They are used in patients with acute coronary events. In those patients with AMI undergoing PCI with a low ejection fraction, they reduced all-cause death.
The CAPRICORN Trial demonstrated that Carvedilol suppressed arrhythmias post AMI.
Lignocaine
Lignocaine is a Class IB antiarrhythmic and blocks fast Na channels. It decreases conduction velocity, which may reduce arrhythmias. Although the evidence is conflicting as it may also cause polymorphic VT, potentially increase mortality. It should not be used prophylactically, but can be used for sustained VT/VF post MI.
Amiodarone
Amiodarone is a Class III drug. It blocks potassium channels and lengthens the refractory period, which suppresses re-entry. It may also decrease automaticity. However it may not confer any increased survival benefit over beta blockers used post MI.
Medications not to use
Flecainide slows conduction and when used in ischaemia may exacerbate VT/VF.
Sedation
Although not a medication therapy, patients with increased arrhythmias may benefit from deep sedation, as it may decreases sympathetic drive.
Overdrive Pacing
If medications fail to treat, then use overdrive pacing.
References
- Mehta RH, et al. Prognostic significance of postprocedural sustained ventricular tachycardia or fibrillation in patients undergoing primary percutaneous coronary intervention.from the HORIZONS-AMI Trial. Am J Cardiol 2012;109:805–12.
- Alexander JH, et al. The GUSTO-I and GUSTO-IIb Investigators. Prophylactic lidocaine use in acute myocardial infarction: incidence and outcomes from two international trials. Am Heart J 1999;137:799–805.
- Huang BT, et al. Meta-analysis of relation between oral b-blocker therapy and outcomes in patients with acute myocardial infarction who underwent percutaneous coronary intervention. Am J Cardiol 2015;115:1529–38
- McMurray J, et al. Antiarrhythmic effect of carvedilol after acute myocardial infarction results of the carvedilol post-infarct survival control in left ventricular dysfunction.CAPRICORN) Trial. J Am Coll Cardiol 2005;45:525–30.
- Zipes DP, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death-executive summary. Europace 2006;8:746–837.
- Boutitie F, et al. Amiodarone interaction with beta-blockers: analysis of the merged EMIAT and CAMIAT databases. Circulation 1999;99:2269–75.
- Zipes DP, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death-executive summary. Europace 2006;8:746–837.
- Sheldon, S et al. Premature Ventricular Contractions and Non-sustained Ventricular Tachycardia: Association with Sudden Cardiac Death, Risk Stratification, and Management Strategies. Indian pacing and electrophysiology journal. 2010, 10. 357-71.
- Riera AR, et al. Accelerated idioventricular rhythm:history and chronology of the main discoveries. Indian Pacing Electrophysiol J. 2010;10(1):40-48







