Adrenaline in Cardiac Arrest may provide no benefit above BLS alone.
Adrenaline is the most frequently used drug in cardiac arrest. It is used to increase arterial blood pressure, as we know that CPR alone, can at best only provide 50% of normal cardiac output.
Adrenaline has both alpha1 and 2 and beta 1 and 2 effects, which can be both beneficial and deleterious. The alpha effects cause a peripheral vasoconstriction which results in blood being shunted to the central circulation. This results in an increase in aortic diastolic blood pressure, which improves cardiac muscle perfusion during cardiac compressions. These alpha effects can also cause constriction of arterioles, which can impair microvascular flow in the cerebral circulation increasing the severity of cerebral ischaemia. They can also stimulate platelet activation leading to thrombus formation. The beta effects increase heart rate and contractility, but also increase myocardial oxygen demand and can cause arrhythmias, all resulting in recurrent cardiac arrest.
Does Adrenaline in Cardiac Arrest increase Survival?
The original studies leading to its recommendation in the ‘Standards for Cardiopulmonary Resuscitation in 1974 (1), were conducted in the 1960’s (2). It was found that adrenaline improved survival in asphyxia in dogs. Currently the guidelines recommend that we give adrenaline at a dose of 1mg every 3-5 minutes during resuscitation.
Although it has been the mainstay of ACLS treatment, evidence showing survival to discharge with good neurological outcome is lacking. In fact, its effectiveness has been found to be no better than BLS alone. Olasveengen (3) compared BLS (CPR and defibrillation) with the use of adrenaline and although it increased short term survival, it also resulted in worst neurological outcomes.
Similar results were published years later in the PARAMEDIC-2 trial (4). This was a multicenter, randomised double blind, placebo controlled trial with 8103 patients.
Primary outcome was rate of survival to 30 days.
Secondary outcomes included:
- rate of survival to admission
- length of stay in hospital and ICU
- rate of survival to hospital discharge
- neurological outcomes at discharge and at 3 months.
The PARAMEDIC-2 Trial found a significant difference, in rate of survival at 30 days that favoured adrenaline (3.2% vs 2.4%). Patients in the adrenaline arm had increased ROSC, and were more likely to be transported to hospital and admitted to ICU. However there was no significant difference in hospital discharge with a favourable neurological outcome.
The number needed to treat with adrenaline to prevent one patient death was 112. However, there were twice the number of patients with severe neurological impairment in the surviving group.
Hagihara (5), in a prospective observational study in Japan, with over 400,000 patients found a positive association with adrenaline use and ROSC and a significant negative association with one month survival and neurological survival.
Jacobs (6) in a double-blind randomised controlled trial, found similarly, that although adrenaline increased ROSC, there was no improvement to neurologically intact survivors to hospital discharge. Unfortunately, this trial was underpowered due to political influence, reducing the number of recruited patients from the original planned 5000 to 534.
Dumas (7) in an observational study found similar results ie., that adrenaline was associated with a decrease in neurologically intact survivors, in patients achieving ROSC (Figure 1).
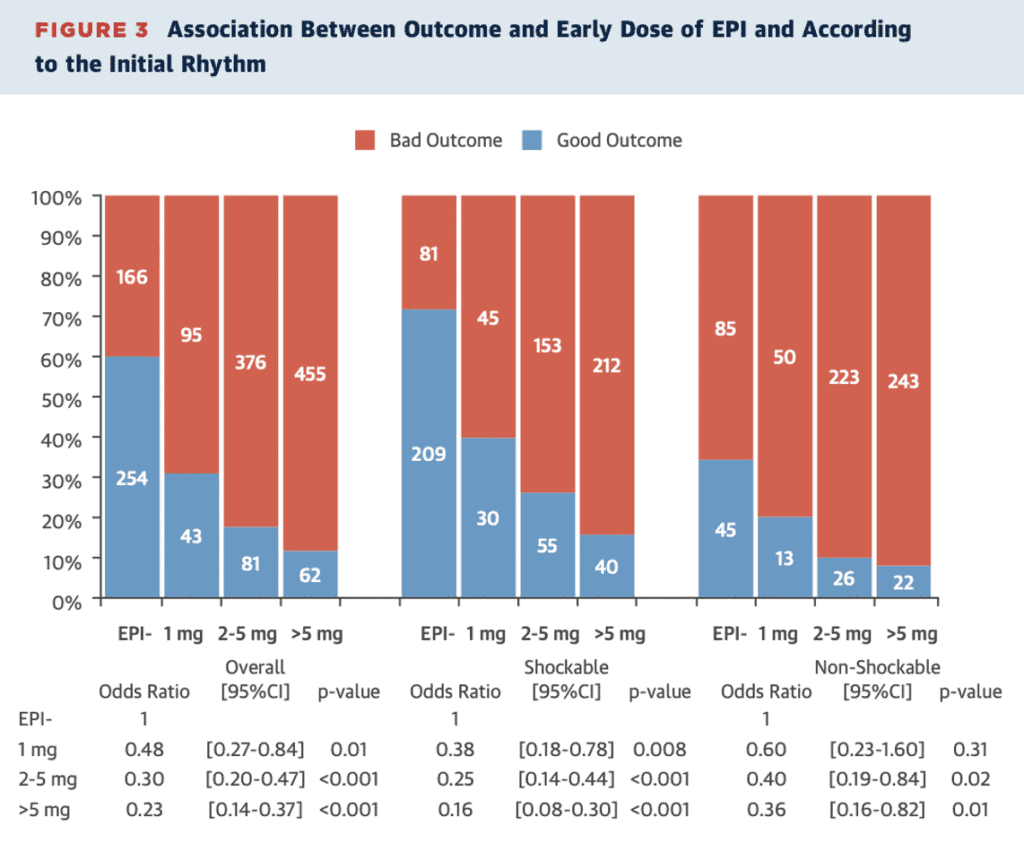
Dumas further found that if the first dose of adrenaline was given within 9 minutes, there was a better chance of survival that if given later. High dose adrenaline (>5mg) led to worst survival.
High-dose adrenaline, is also associated with a higher level of myocardial dysfunction following ROSC and although it is shown to increase ROSC, it does not improve neurological outcome in surviving patients (8). In 2000 high dose adrenaline was no longer recommended for use during cardiac resuscitation.
Does Low Dose Adrenaline Work?
Fisk (9) looked at out of hospital cardiac arrest in 2255 patients and found that a lower dose of adrenaline was not associated with survival to discharge or favourable neurological outcome.
Does Timing of Adrenaline Matter?
Dumas(7) found that early administration improved survival. Ran (10) found that early administration ie., at <10 minutes resulted in patients being 3.21 times more likely to have a favourable neurological outcome than those receiving it at greater than 10 minutes. Overall early administration of adrenaline was associated with:
- Increased survival to discharge
- Overall ROSC
- Favourable neurological outcome.
The success of adrenaline administered early may relate to Weisfeldt’s (11), 3 phases of resuscitation.
- The Electrical Phase: This occurs in the first few minutes of arrest. Adrenaline should not be required here.
- The Circulatory Phase: Chest compressions and adrenaline may help perfusion
- The Metabolic Phase: Adrenaline is detrimental in respect to peripheral ischaemia releasing cytotoxic proteins.
Removing the beta Effects of Adrenaline……enter Vasopressin
Vasopressin is a potent, pure vasoconstrictor. Porcine model studies, in the 1990’s compared Vasopressin to adrenaline and normal saline (12) and found an increased survival and full neurological recovery in the vasopressin group.
Following this, in 2000, Vasopressin was recommended in the AHA guidelines and remained a recommendation until 2015.
A review of trials of Vasopressin use in humans (13) in 2014, found that there was no benefit in terms of ROSC, survival to hospital discharge or favourable neurological outcome. Following this the recommendation for the use of Vasopressin was withdrawn. This study did show however, that for in-hospital cardiac arrest, when used in repeated doses titrating to effect, it was associated with higher possibility of survival and favourable neurological outcome.
Can we use NorArenaline in Cardiac Arrest?
There are very few studies looking at noradrenaline during cardiac arrest. Most of the work relates to post arrest shock.
Patient mortality in ICU following cardiac arrest, tend to be due to neurological injury or haemodynamic failure. A recent randomised controlled trial (14) comparing adrenaline with noradrenaline, showed no difference in overall mortality, but was terminated early due to the higher incidence of refractory shock in the adrenaline group.
In post cardiac arrest shock a recent observational multicenter study found that adrenaline had a significant increase in all cause cardiovascular mortality (15).
When comparing the haemodynamics of noradrenaline and adrenaline during CPR in a porcine mode, Robinson et al (16) found that there was a trend towards improved myocardial blood flow and successful defibrillation rates with noradrenaline.
Tortolani et al(17) compared adrenaline to noradrenaline and lignocaine in a retrospective study of 123 patients with in hospital cardiac arrest and an initial rhythm of asystole and found patients receiving noradrenaline were more like to survive (39.5% vs 14.1%). Further they found that the patients receiving noradrenaline and lignocaine had the best survival rate. They proposed that the mechanism for this was the peripheral vasoconstriction of noradrenaline and the suppression of automaticity by lignocaine.
In a randomised prospective double blind trial comparing high dose adrenaline with high dose noradrenaline in 816 patients, it was found that high dose adrenaline did not result in better outcome, and it was also found that high dose noradrenaline did not result in increased survival (18).
Those receiving high dose adrenaline and noradrenaline had the worst neurological outcome (perhaps not unexpectantly).
There is a lack of studies looking at Noradrenaline.
Conclusion
Adrenaline does not result in better survival than BLS alone. Although it does increase the rate of ROSC, it is associated with worst neurological outcomes. The one exception is early administration.
Different doses don’t change this outcome. The timing of adrenaline may affect survival.
Alternatives to adrenaline including Vasopressin and Noradrenaline, don’t perform any better.
Perhaps we should use a two drug strategy, using adrenaline in the first 10 minutes post arrest and then switch to noradrenaline. Perhaps it’s time to remove adrenaline altogether, rather than testing different alternatives of a drug that doesn’t seem to work.
We want it to work but…….. Perhaps the time is right for a total paradigm shift.
Personally I use 3 doses of adrenaline and then stop.
References
- Donnino MW et al. American Heart Association’s Get with the Guidelines-Resuscitation Investigators. Time to administration of epinephrine and outcome after in-hospital cardiac arrest with non-shockable rhythms; retrospective analysis of large in-hospital data registry. BMJ. 2014;348:g3028
- Redding Js. Et al. Resuscitation from asphyxia. JAMA 1962;182: 283-286.
- Olasveengen TM et al. Outcome when adrenaline was actually given vs not given- post hoc analysis of a randomised clinical trial. Resuscitation 2012;83:327-332.
- Perkins GD et al. A Randomised Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. NEJM 2018; 379:711-21
- Hagihara A et al. Prehospital epinephrine use and Survival Among Patients with Out of Hospital Cardiac Arrest. JAMA 2012;307:1161-8
- Jacobs IG et al. Effect of adrenaline on survival in out of hospital cardiac arrest: A randomised, double-blind, placebo-controlled trial. Resuscitation 2011;82:1138-43
- Dumas F et al. Is Epinephrine During Cardiac Arrest Associated with worse Outcomes in Resuscitated Patients? JACC 2014;64:2360-7
- Lin S et al. Adrenaline for out-of-hospital cardiac arrest resuscitation: a systematic review and meta-analysis of randomised control trials. Resuscitation 2014;85:732-40.
- Fisk CA et al. Lower-dose epinephrine administration and out-of hospital cardiac arrest outcomes. Resuscitation 2018;124:43-8
- Ran L et al. Early Administration of Adrenaline for Out-of-Hospital Cardiac Arrest: A Systematic review and Meta-Analysis. J Am heart Ass 2020;9:e014330
- Weisfeldt ML et al. Resuscitation after cardiac arrest: 3 phase time-sensitive model. JAMA 2002;288:3035-8
- Wenzel V et al. Survival with full neurological recovery and no cerebral pathology after prolonged cardiopulmonary resuscitation with vasopressin in pigs. JACC 2000;35:527-533.
- Layete A et al. Efficacy of vasopressin during cardiopulmonary resuscitation in adult patients: a metaanalysis. Resuscitation 2014;85:853-863
- Levy B et al. Epinephrine versus norepinephrine for cardiogenic shock after acute myocardial infarction. JACC 2018;32:173-182.
- Bougouin W et al. Epinephrine versus norepinephrine in cardiac arrest patients with post resuscitation shock. Int Care Med 2022;48:300-310.
- Robinson et al. The effect of norepinephrine versus epinephrine in myocardial hemodynamics during CPR. Ann of Emer Med 1989;18:336-340.
- Tortolani A et al. In-hospital cardiopulmonary Resuscitation during Asystole: Therapeutic Factors associated with 24-hour survival. Chest 1989;96:622-626.
- Callaham M et al. Randomised Clinical trial of High Dose Epinephrine and Norepinephrine vs Standard -Dose Epinephrine in Prehospital Cardiac Arrest. JAMA 1992;268:2667-2672.







