A 59 yo male presents to the Emergency Department, 5 days post ablation for atrial fibrillation. He is complaining of dizziness and nausea. He is also seeing spots before his eyes.
He has no other past medical history and is on a DOAC and Sotalol
His BP is 122/68 with no postural drop and his pulse rate is 49 bpm.
His ECG is shown below. What does the ECG show? (HINT: The exam is the key)
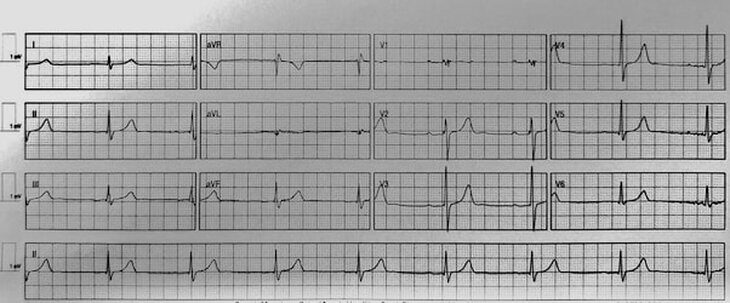
The ECG is sinus bradycardia at a rate of 49 with a first degree block. Not much to see.
The examination showed:
- Dual Heart Sounds, with no extra sounds
- Chest clear
- Abdomen soft
- Given his dizziness, his neurological examination as per the ‘Dizzy Patient’ algorithm on the RESUS blog.
- His Cranial Nerve exam showed
- No nystagmus, no diplopia and pupils equal and reactive.
- On visual fields he stated he saw some spots before his eyes but no ‘floaters’. He also stated that in his peripheral vision he saw a ‘kaleidoscope’ pattern of colours.
- Fundoscopy was normal
- Facial nerve examination was normal and there was no speech disturbance
- Given that he had no nystagmus, head impulse test was fruitless to do, but done anyway and was negative. Dix-Hallpike was also performed and was normal.
- Cerebellar examination was normal
- Upper and lower limb neurological examination was normal
- His Cranial Nerve exam showed
What’s the diagnosis?
I’ll add that I did a non-contrast CT brain on him, purely because he was on a DOAC. This was normal.
Approximately one hour later the patient had improved and felt well.
What’s your initial thinking and diagnosis?
My initial thinking was as follows:
- This might be Sotalol related, as it can produce dizziness and nausea. Alternatively the dose he was on (80mg bd) may have been too high.
- Second thought was that this might be a peripheral vestibulopathy, but all the examinations were normal, head impulse test and Dix-Hallpike. Also with no nystagmus and dizziness, a central cause should be more likely.
- Could this be a bleed, because he was on a DOAC?
- It didn’t sound like a stroke.
- The kaleidoscope colours and spots before his eyes sounded like a migraine, but he was not a migraine sufferer.
I initially spoke with the neurologist who agreed that it sounded migrainous and did not think he needed an MRI. I then spoke with his electrophysiologist ….
“I’ve got Mr X with us, who had the ablation 5 days ago. He’s come in with nausea and dizziness. His ECG is normal and he is haemodynamically fine. His neurological exam looking for a peripheral or central cause is normal. The only thing I can say is that he has this kaleidoscope vision and to me, this points to a migraine, but he isn’t a migraine sufferer.”
The Diagnosis
The electrophysiologist said “This is a post ablation migraine”.
The literature shows that a percentage of patients, up to 2%, (thought to be even higher), present with migraines, usually with no headache but aura and visual disturbances. These visual disturbances include scotomas and scintillating edges to vision. Attacks occur within one week of the ablation and usually resolve within 3 months.
The reason appears to be that during catheter ablation for atrial fibrillation, a transeptal puncture is required to provide access to the left atrium. This provides access to the pulmonary veins. The result is that it creates a transient right to left shunt.
The exact mechanism for why this might then occur is unknown, but can include factors usually cleared by the lungs, now reaching the cerebral circulation, and even microemboli. It is usually transient and no specific treatment is needed if there is no neurology and the patient is on anticoagulation. If abnormal neurology is found, then the patient should definitely be discussed with neurology.
We see a lot of post ablation patients, given that atrial fibrillation is now becoming such a massive arrhythmia burden, that we will see post ablation migraines.
The patient was well and all symptoms (which did not involve any significant neurology) had resolved, he was discharged, to be reviewed by his cardiologist.
References
- Noheria A et al. Migraine headaches following catheter ablation for atrial fibrillation. Journal of Interventional Cardiac Electrophysiology 2011; 30:227–232
- Kato Y et al. Migraine-like Headache after Transseptal Puncture for Catheter Ablation: A Case Report and Review of the Literature. Intern Med 2019;58(16):2393-2395







