The patient with vertigo can be a clinical challenge. Patients may describe their symptoms as vertigo, or the room spinning, or dizziness, or a problem with balance, or use other descriptors. Trying to understand the patient’s symptoms can be difficult and we know that asking questions about rapidity of onset, duration and triggers may be more helpful to us.
There are a lack of clinical decision guidelines to provide a standard approach to the patient who presents with vertigo or dizziness. This results in variations in diagnostic approach, including the need for investigations, especially neuroimaging. For example, up to 50% of patients with vertigo undergo a CT brain, most of which are normal.
What do we currently have in terms of Risk Scores?
- The Head Impulse, Nystagmus, and Test of Skew (HINTS) examination. It is used for those patients with acute vestibular syndrome (ie., the patient must have vertigo and nystagmus).
- STANDING algorithm: This is an assessment of Nystagmus and if it is spontaneous or triggered and uses the head impulse test. Its sensitivity has been reported at 93%.
- The TriAGe+ score has 8 variables (sensitivity of 96.4%):
- triggers,
- atrial fibrillation,
- male,
- hypertension,
- brainstem or cerebellar dysfunction,
- focal weakness or
- speech impairment,
- dizziness with no history of vertigo. External validation of this score yielded a .
- The stroke-risk assessment nomogram uses sex, trigger, isolated symptoms, nausea, history of brief dizziness, high blood pressure, finger–nose test, and tandem gait assessment. This had a high diagnostic accuracy.
- The DEFENSIVE stroke scale uses sensory disturbance, ataxia, and visual deficit.
We review the following study still in press, which proposes a new score; The Sudbury Vertigo Risk Score:
Ohle R, et al. Development of a Clinical Risk Score to Risk Stratify for a Serious Cause of Vertigo in Patients Presenting to the Emergency Department. https://doi.org/10.1016/j.annemergmed.2024.06.003. Article in Press.
The aim of this study was “to prospectively assess the clinical characteristics of patients presenting with vertigo to the ED and to derive a clinical risk score to identify high- and low-risk patients for a serious cause of their vertigo.”
What They Did
This was a prospective multicenter cohort study, conducted in three Canadian Emergency Departments. It included adult patients ( > 17 yo) presenting with acute vertigo, dizziness, or imbalance.
Patients were excluded if:
- Symptom onset was more than 14 days prior
- There had been head or neck trauma in the preceding 14 days
- Glasgow Coma Scale score was less than 15
- Systolic blood pressure was less than 90 mm Hg
- A syncopal episode had occurred in the preceding 14 days
- Active cancer was present
Physicians completed data forms to identify the presence or absence of 67 clinical findings, which included history and clinical examination findings.
Telephone follow-up calls were conducted at 7, 30, and 90 days to assess if the patient had a diagnosis of stroke, TIAs, vertebral artery dissection, or brain tumor diagnoses. A validated tool, the Questionnaire for Verifying Stroke-Free Status was used for outcomes.
N= 2078
Primary Outcome was a diagnosis of stroke, TIA, vertebral artery dissection, or brain tumor diagnosed in the ED or within 30 days of the initial assessment.
What They Found
Some of the initial findings included:
- Mean age was 77.1 years of which 59% were women
- CT head scan was performed in 643 (30.9%) patients
- MRI scan was performed in 56 (2.5%) patients
- 160 (7.7%) patients were admitted to the hospital
- Specialist consultation occurred (ED or outpatients)for 234 (11.3%) patients.
- There were 111 (5.3%) serious diagnoses, including:
- 99 cases of stroke (81.1%),
- 11 cases of TIAs (9.9%),
- 2 cases of vertebral artery dissection (1.8%),
- 1 brain tumor (0.9%).
Follow-up was complete for 80.4% of the cohort at 30 days.
Clinical features found to strongly correlate with having a serious cause of vertigo included:
- sex,
- age > 65 years,
- mean systolic blood pressure (157 mm Hg),
- previous stroke or TIA,
- hypertension,
- diabetes,
- dysphagia,
- diplopia,
- motor / sensory deficit,
- ataxia,
- dysarthria,
- dysmetria,
- headache,
- unable to walk unaided,
- ongoing dizziness,
- dizziness lasting more than 2 minutes, or
- a single episode of dizziness.
Features found to be negatively associated with a serious cause included:
- Multiple episodes
- Dizziness triggered by head turning, getting up, lying down, rolling over in bed, or a change in any position
- A diagnosis of benign paroxysmal positional vertigo
Multivariate “analysis found 6 variables independently positively associated and one variable negatively associated with a serious diagnosis. The model had excellent discrimination..”
The Sudbury Vertigo Risk Score has 7 components. The score ranges from -4 to 17.

Probability of a serious cause
- 0% for a score of <5,
- 2.1% for a score of 5 to 8, and
- 41% for a score >8
Using the score for the primary outcome; sensitivity was 100% (95% CI 97-100%) and the specificity was 72.1% (95% CI 70.1% to 74%) for a score >4.
My Take On This
Firstly there are some limitations to this study:
- All eligible patients were not enrolled.
- This was a Canadian study in three emergency departments. It needs external validation as the results may not be applicable to different countries and even different emergency department setting ie., rural departments.
- The variables were applied by Emergency Physicians or trained Residents. We are not sure what the results would be in an department where specific training is not undertaken.
- 19.6% of patients did not have followup data. Although none of those patients had neurologic deficits, strokes may have been missed as not all patients present with neurological symptoms.
We need a validation study on this. My greatest concern with scores like this is that if we apply them indiscriminately, we may discharge patients inappropriately, or investigate more patients. This is similar to performing a heart score, where we can get a low risk score even with a positive troponin, however we won’t necessarily be considering a patient with a high troponin as low risk.
In a score such as this, there are three things I consider important:
- If I can rule in BPPV, then my diagnosis is a peripheral cause and I’m done;
- If the patient has neurological findings then I’m done and that patients needs neurological referral and probably an MRI.
- If the patient has no symptoms now and I purely base my approach on a score like this ie., using risk factors, then a 66 yo male with a past history of diabetes and hypertension, will score a 6, which is not low risk and this may lead to more neuroimaging. Will this be the answer? We won’t know until a validation study is done.
My approach is still centred around the following:
- Determine if the episode is recurrent or prolonged
- If it’s recurrent I want to know if it’s spontaneous or triggered
- If it’s spontaneous I think of:
- Menier’s Disease: Hearing loss, Tinnitus, Vertigo, Drop Attacks
- Vestibular Migraine: Family History, Migraine associated in > 2 episodes
- Laryrinthitis: Recent infection, hearing loss
- If it’s triggered I think of:
- BPPV: Short duration, positional, +ve Dix Hallpike, +ve Supine roll test
- If it’s spontaneous I think of:
- If it’s prolonged I think of:
- Acute vestibular neuronitis: Gradual onset and +ve head impulse test (Watch a Head Impulse Test)
- Cerebellar causes: Sudden onset and -ve head impulse test
- If it’s recurrent I want to know if it’s spontaneous or triggered
- Is there any positive neurology except a +ve Rhomberg or Head Impulse Test? if so, it’s central. The neurological examination must include:
- Speech
- Cranial Nerves: Eyes: III, IV, VI, Nystagmus and Brainstem VII, VIII, IX, X
- The 5 D’s: Diplopia, Dysmetria (+gait), Dysarthria, Dysphonia, Dysphagia
- Upper and Lower limb neurological examination
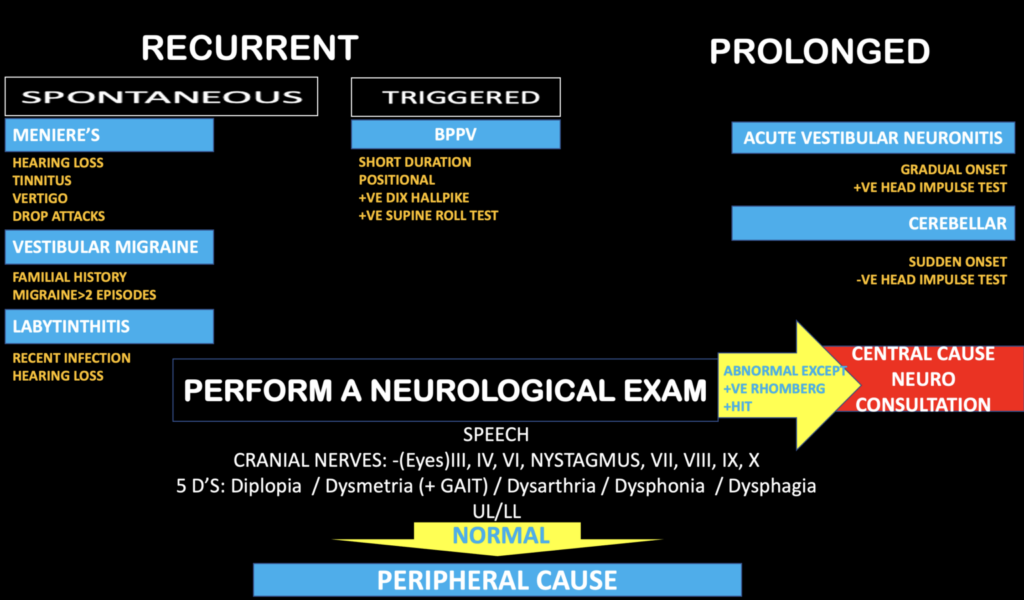
Approach to the dizzy patient
References
- Jones WJ, et al. Validating the Questionnaire for Verifying Stroke-Free Status (QVSFS) by neurological history and examination. Stroke. 2001;32:2232-2236.
- Kattah JC, et al. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke. 2009;40:3504-3510.
- Vanni S, et al. STANDING, a four-step bedside algorithm for differential diagnosis of acute vertigo in the Emergency Department. Acta Otorhinolaryngol Ital. 2014;34:419-426.
- Kuroda R, et al. The TriAGe+ score for vertigo or dizziness: a diagnostic model for stroke in the emergency department. J Stroke Cerebrovasc Dis. 2017;26:1144-1153.
- Bi Y, et al. A dynamic nomogram to predict the risk of stroke in emergency department patients with acute dizziness. Front Neurol. 2022;13; 839042-839042.
- Yamada S, et al. DEFENSIVE Stroke Scale: novel diagnostic tool for predicting posterior circulation infarction in the emergency department. J Stroke Cerebrovasc Dis. 2019;28:1561-1570.







