
The ECG is usually quite straightforward to analyse if we remember 2 things:
- The T waves are upright in the first week of life. They are inverted after this until about age 9-10
- When a child is born, they are right heart dominant. As they grow older, they become more left heart dominant.
Any neonate or infant presenting with difficulty feeding, or shortness of breath whilst feeding, or change of colour whilst feeding, needs to be examined for a potential heart condition.
In any child presenting this way, we need to think of:
- VSD
- Tetralogy of Fallot
- Myocarditis
- Cardiomyopathy
- Arrhythmia.
It is also useful to have an idea of heart rates at various age groupings. My rough guide is:
- < 2yo max 160
- 2 – 7yo max 140
- 7 – 15 yo max 130
Here is the approach as per the ‘ECG in 20 Seconds’
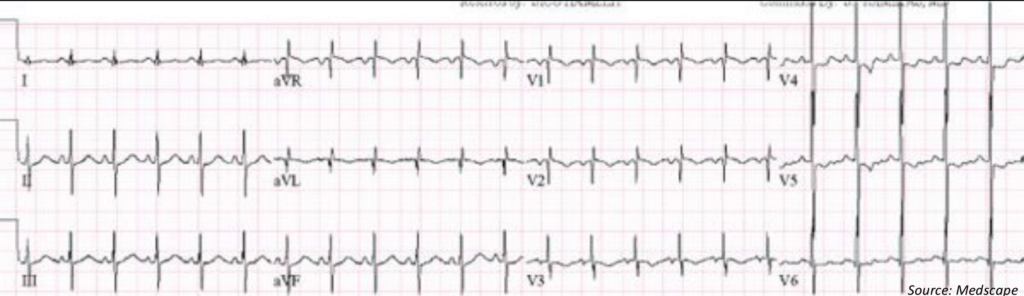
Rate: just count the number of complexes and multiply by 6 ( an ECG takes 10 seconds to print). Rate = 23 x 6 = 138, which is acceptable
Rhythm: For sinus rhythm, there must be a P wave before each QRS and the P wave must be upright in II and inverted in aVR. If not, then it is not sinus rhythm and the pacemaker is in the low right/left atrium
This is sinus rhythm
QRS: is it too tall or too small, ie is there hypertrophy? Remember that in the child the is right ventricle is dominant. To judge hypertrophy look at V6. If the R wave intersects the baseline of the V5 tracing above, then there is LVH
In terms of Right Ventricular Hypertrophy, in adults it is usually hidden by the left ventricle, however in children the clues are in V1. There is RVH if there is an rsR pattern in V1, or a pure R wave in V1 after 6 months.
It is also helpful to look at the R wave to S wave ratio. Remember that the young heart is right heart dominant, so you would expect that the R wave is more predominant than the S wave in the right leads, however if the opposite is true, then there is left ventricular hypertrophy.
The QRS is normally +ve in aVF
- If it is negative in aVF, there may be cardiac malformations, such as AV septal defect.
- If it is biphasic in aVF, it may be normal, but needs cardiology discussion.
Look for the abnormal QRS morphology i.e.., the delta wave of WPW
This shows Left Ventricular Hypertrophy. The heart is left heart dominant rather than right heart dominant, which we would expect in this age group. With the murmur and the crepitations and the left heart dominance, this is most likely VSD(left to right shunt).
ST-T: The T wave is upright for the first week of life, then is inverted until adolescence.
This is normal.
Intervals:
PR- In anyone, an interval > 0.2 sec is abnormal
- In infants and young children an interval of > 0.16 (4 small squares) is abnormal.
QT- >0.45sec is abnormal in anyone
- In < 6 months <0.49sec
- In > 6 months <0.44
It appears that the QTc is quite long here.
This ECG is of a patient with VSD. Paeds referral is needed for further investigation including an Echo and bloods. Treatment may include:
- Oxygen
- Fluid Restriction
- Diuretics
- Ace Inhibitor







