
Below is another example:
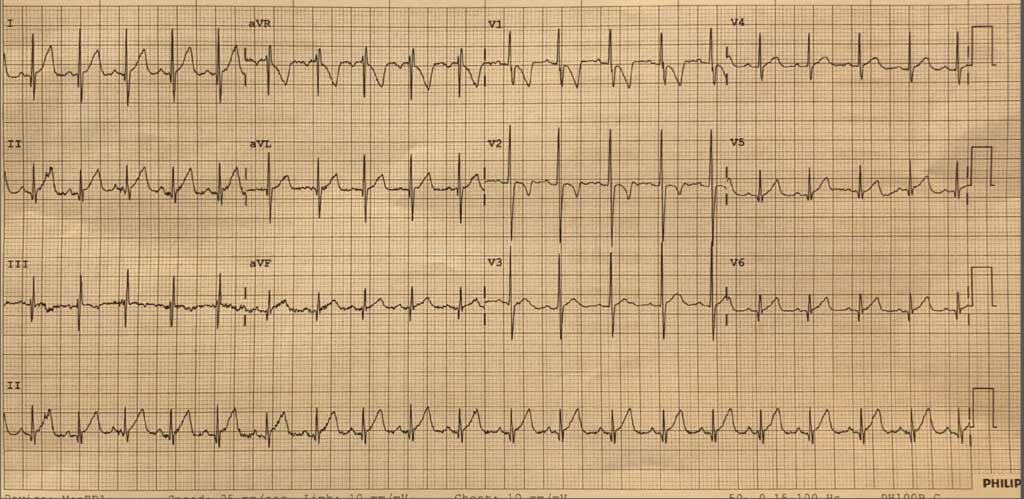
This is someone at a rate of 120bpm. Notice the inverted p’s in lead III. Again, this is unifocal atrial tachycardia.
Clinical Presentation
The usual presentation is one of palpitations, but may be that of syncope, or cardiac failure if the patient has been in the rhythm long enough.
Workup
An ECG and electrolytes to ensure no abnormalities and a full blood count to exclude anaemia.
Very few other investigations are needed in the emergency department. Perhaps a chest xray if lung pathology is suspected. The patient should have an echocardiogram, to look for structural abnormalities, but this can be as an outpatient.
Management
The unifocal atrial tachycardia can be treated like an SVT.
The general treatment for this condition is:
- Pharmacological
- Beta blockers
- Calcium channel blockers
- Cardioversion
In this case we gave the patient his usual dose of Sotalol and waited, however it was clear that there was not going to be resolution, so we proceeded to cardiovert.







