
A 38 yo male presents with sharp stabbing central chest pain. It changes with breathing. He feels worst when he is lying down. He is haemodynamically stable. An ECG is done. What does it show?
WHAT DOES THE ECG SHOW?
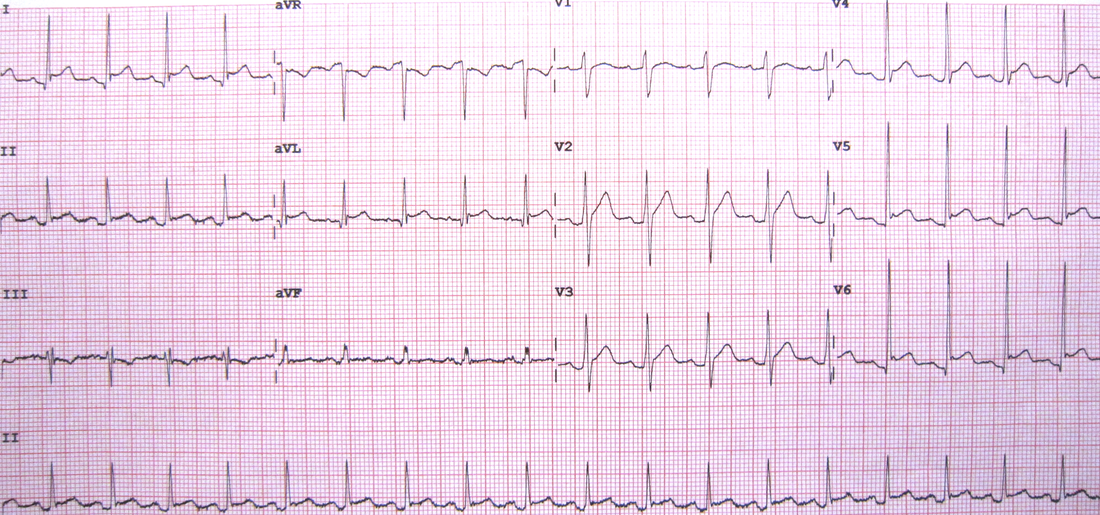
Using the ECG in 20 Seconds Approach:
- There is a sinus tachycardia at about 108bpm
- The P wave is upright in II and inverted in aVR, so it is sinus
- The QRS morphology is normal
- The ST-T segments are not normal:
- There is ST elevation in multiple leads ie., I, II aVL, V4, V5, V6
- There appears to be a J point in aVL, V4, V5 and V6, so Benign early repolarisation is an alternative diagnosis.
- There is ST depression in aVR
- Is that ST depression in III?
- Initially it does look like ST depression, however when we draw in the isoelectric line, it is not really as significant (see below).
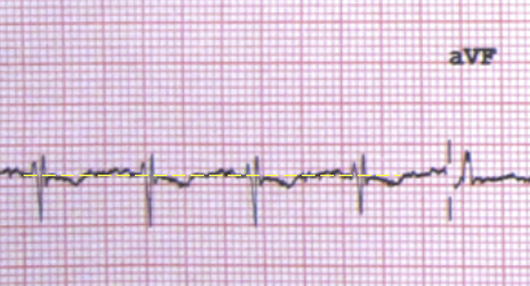
REMEMBER: When looking for ST elevation or depression, use the T-P line as the isoelectric line.
- The QT and PR intervals are normal
- It is obvious that there is PR depression
- There are no pacing spikes
DIAGNOSIS
The diagnosis is most likely pericarditis.
The history is very indicative of that. The characteristics of the pain ie., that is it worst on lying down indicate pericarditis. Although there appears to be a pleuritic component, there is no real other history of a PE and the ECG does not show a right axis or S1Q3T3 etc.
In the ECG itself:
- There is ST elevation, concave in nature
- There is ST depression in aVR, which is allowed ie., there can be ST depression in aVR and V1
- There are no ischaemic looking waveforms and no real reciprocal changes.
- There is PR depression.
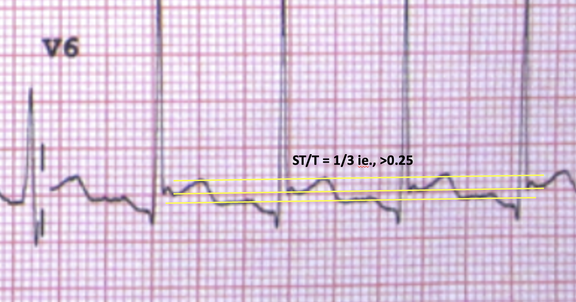
- We can also measure the ST/T ratio. A ratio of >0.25, when put together with all the other parameters indicates pericarditis.
WHAT TO DO NEXT
- Do a bedside echo looking for an effusion. It will also assist to look for wall abnormalities.
- Get a troponin. A slight rise in troponin may be normal. We need to make sure that we don’t miss, perimyocarditis or myocarditis, where we would expect a significant rise in troponin.
Who needs admission and who can be discharged?
What is Spodick’s Sign and how good is it?
What are the stages of Pericarditis?
What is the treatment?
Is there a role for glucocorticoids?
What is Spodick’s Sign and how good is it?
What are the stages of Pericarditis?
What is the treatment?
Is there a role for glucocorticoids?








Hi Peter,
Thank you very much for this interesting and always challenging ECG.
Peter, you did not mention an obvious PR elevation in aVR as one of the ECG features of Pericarditis.
Was this just simple overlooking of something that we always look for or PR elevation in aVR is not relevant.
Cheers
Marin