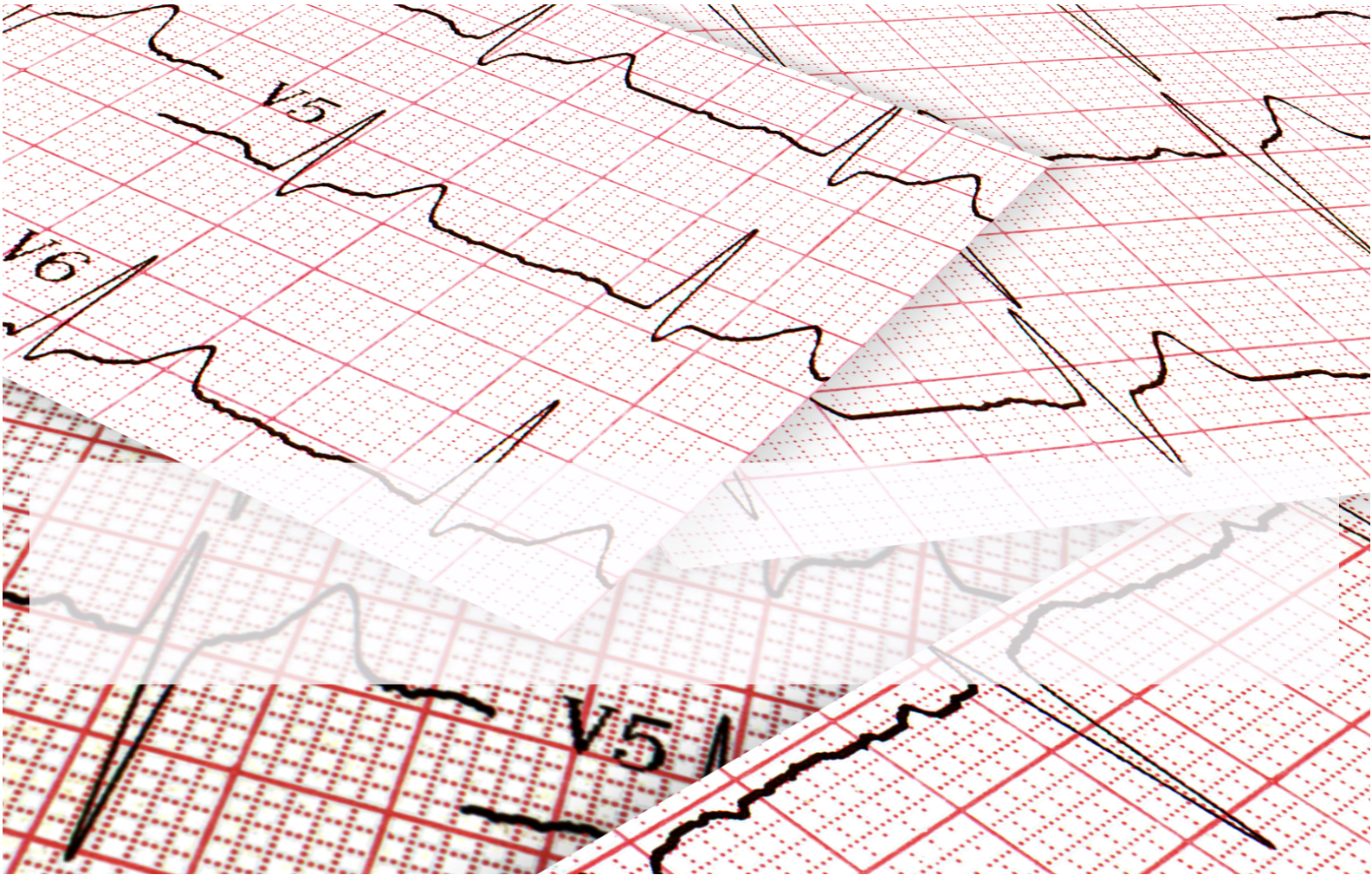
She presents complaining of palpitations different to the ones she normally has with her bigeminy. She is well looking, afebrile, with a blood pressure of 142/70 and a normal respiratory rate. A Venous Blood Gas shows a potassium of 3.3mmol/L. Her ECG is as below.
What is the Diagnosis and how would you Manage this patient?

ECG INTERPRETATION
It is a wide complex tachycardia. The rate is about 1`50bpm and I think I can see ‘p’ waves in lead I. In a well young person, we might assume it’s SVT. Could it be VT? It could be.
The patient is young so SVT with aberrancy is probably most likely. However we need to be a little bit careful with that. Ventricular bigeminy can lead to arrhythmias.
The patient is stable and looks well, so we have some time to think.
IS IT VENTRICULAR TACHYCARDIA?
We know that 80% of wide complex tachycardias are Ventricular Tachycardia(1). There are well known rules that we can use. Let’s see what happens if we use them.
BRUGADA CRITERIA(2)
The Brigade Criteria are 92% sensitive and 65% specific, so not perfect. There are 4 parts:
- Is there an absence of an RS complex in all precordial leads? NO
- R-S Interval >100ms in any precordial lead? YES– indicating VT, so we can stop here.
- Why is the RS interval important? It tells us that there is a delay in the impulse propagating, which occurs if it passes through the ventricle instead of the AV node.
VERECKEI CRITERIA(3)
The Vereckei Criteria have similar sensitivity to Brugada. Let’s apply Vereckei:
- Is there AV Dissociation? NO
- Is there a dominant R wave in aVR? YES indicating it is VT
GRIFFITH CRITERIA.
Griffith Criteria having about the same sensitivity, but rule in SVT.
It’s all too complex. In the real world cardiologists reviewing these eggs can’t agree.
WHAT IF WE ASSUMED IT WAS SVT AND GAVE ADENOSINE?
If it’s ventricular tachycardia, apart from a particular kind of ventricular tachycardia, then nothing would happen, as Adenosine blocks the AV node and Ventricular tachycardia comes form the Ventricles. You wouldn’t harm the patient unless it were an irregular wide rhythm (ie., AF with WPW)
We need a simple solution to working this out. We need a solution that you can apply when you’re woken at 2 o’clock in the morning.
MY 3 STEP APPROACH
- Is the QRS wider than 120ms(3 small squares)?
- Is the Rate greater than 120?
- The rate must be greater than 120 beats otherwise think of 3 other differentials”
- Hyperkalaemia
- Na Channel Blockade
- Accelerated Idioventricular Rhythm.
- The rate must be greater than 120 beats otherwise think of 3 other differentials”
- Is this real? i.e. is it not artefacts etc.
If the answer is yes to all 3 questions, go down the VT route. Use electricity. 200J on this patient following consent and sedation.
What would I do in this case?
Given the patient is stable and looks well, I would try a vagal manoeuvre, either the ‘REVERT‘ technique, or the ‘Reverse Vagal Manoeuvre‘. If these were not successful, I would advise the patient on the side effects of Adenosine and try Adenosine. If the blood pressure dropped at any point I would prepare for cardioversion, but would give a small dose of Metaraminol, as this sometimes reverts SVT.
Always check the POTASSIUM in any arrhythmia
A final word about bigeminy. I recently wrote a blog on this topic on resus.com.au titled ‘Is Bigeminy Benign?‘ The bottom line is that we normally don’t need to do anything for these patients, as ectopics are a normal physiological response.
HOWEVER:
- In patients with ischaemic heart disease, these may be significant and caused by the ischaemia. Beware the multiple premature ventricular ectopics in MI.
- Beware premature ventricular contractions(PVC’s) and Long QTc as this may predispose to R on T phenomenon. The premature complex may fall on the T wave resulting in Torsades de Pointes.
References
- Zipes D P et al. Circulation 2006; 114(10) e 385-484
- Vereckei A et al. European Heart Journal, Volume 28, Issue 5, 1 March 2007, Pages 589–600
- Brugada et al Circulation Vol 83, No 5 May 1991. 1649-1659









I recently say a 55 yo male dz with low BP.
Hr 175 wide complex
I cardioverted him (unstable) with 200j and he went asystole
Short burst of cpr and the VT which I defib and got him back.
He later signed out AMA. I love your work
Thanks