The patient is haemodynamically stable.
An ECG is done and there is concern over the rate.
Look at the ECG. What is the diagnosis?
Is it SVT? Is it Torsades? What do you do next?
………Move away from the patient….. ie., do nothing. Let’s see why.
Let’s go back to the clinical picture.
The patient is haemodynamically stable and looks well.
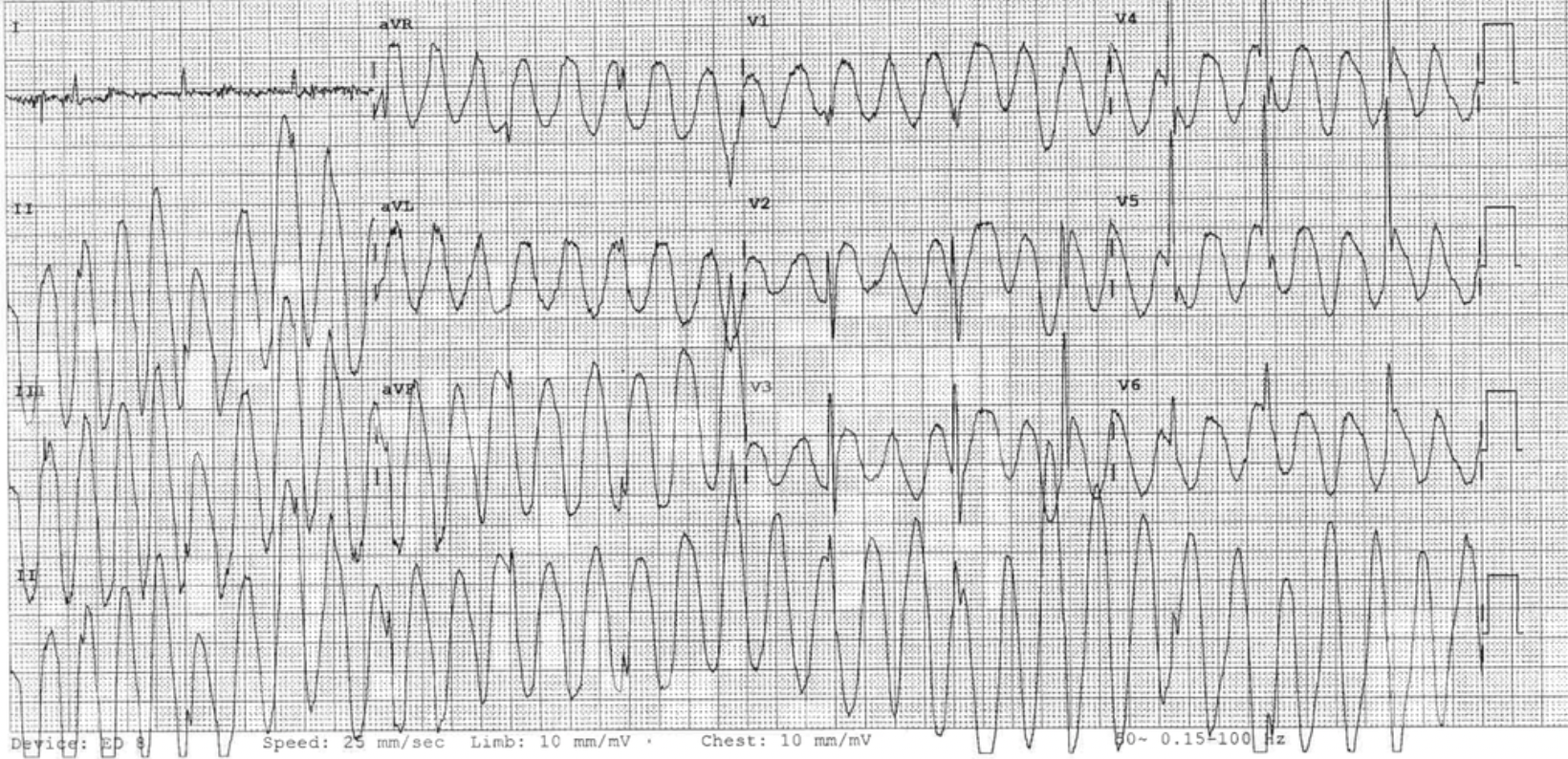
Now back to the ECG: It is a narrow complex EXTREME tachycardia.
Notice lead III. It is not the same as the others. One lead cannot refuse to show the tachycardia whilst all the others are. In fact lead III here is the underlying rhythm. The rest of the ECG is artifact.
Remember that if the ventricle is beating at above 300 beats per minute in an adult patient, it will very soon convert to ventricular fibrillation.
Clinically at a rate of 350 or so, the patient will not be stable, as the ventricle doesn’t have time to fill properly, so the blood pressure will be impaired.
What is the artifact caused by?
Artifacts can be external, relating to line current. They can also be internal relating to tremor or shivering. They can also be caused by other devices such as deep brain stimulators ( which are usually there to control tremor).
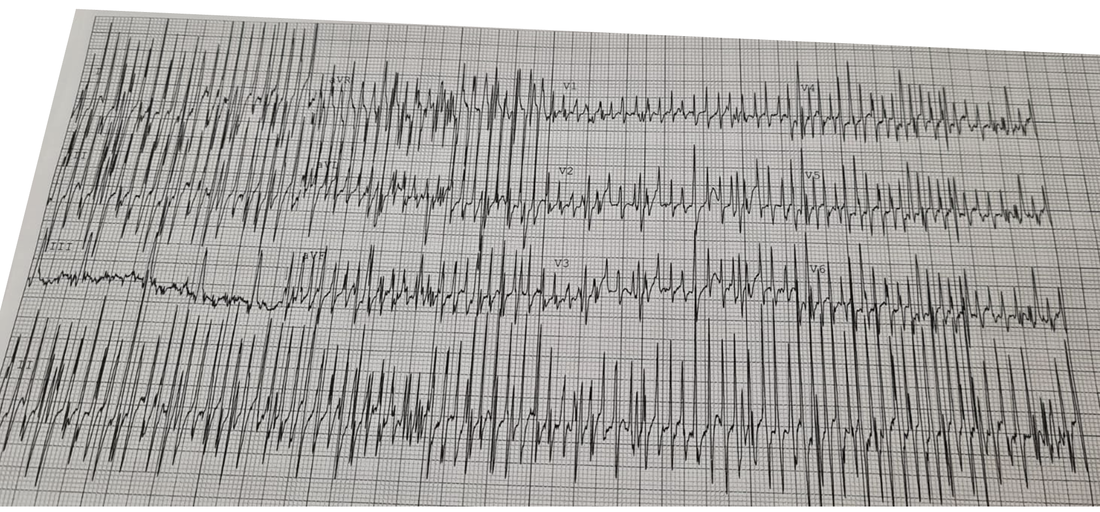
An ECG was redone and is shown below. The artifact is gone and the patients underlying rhythm is there.

To read more on this and see more examples like the one below go to the blog on ‘A Patient with Wide Complex Tachycardia’