
An 81 yo male presents to triage with chest pain. The pain started last evening ie., 14 hours previously and is still present.
The pain is described as a pressure pain with some radiation into the jaw area. There is no diaphoresis, no dyspnoea and no distress.
There is minimal past medical history.
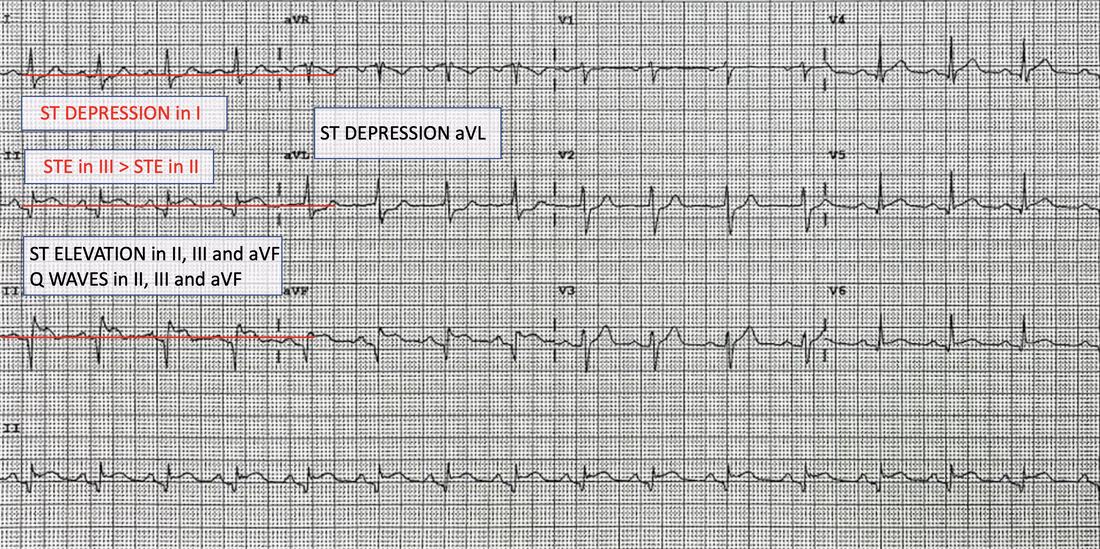
An ECG is done. Take a moment to look at it.
QUESTION: What does it show?

ANSWER: There is an INFERIOR infarct. In most cases this is due to a RIGHT CORONARY ARTERY occlusion but in a small number of cases a left circumflex artery occlusion can also cause this.
A right coronary occlusion is most likely as when the following are present:
- STE in III > STE in II and
- there is some ST depression in I (see below).
If this were a circumflex lesion, these changes would not have occurred.
The patient gets ASPIRIN and you prepare to give GTN.
QUESTION: Should you give GTN? What ECG should you perform before this?
ANSWER: We know that up to half of all patients with an inferior infarction will develop RIGHT VENTRICULAR infarction. Right Ventricular infarction is associated with a greater than two-fold increase in mortality as well as an increased risk of arrhythmias and high grade AV-nodal blocks.
Patients with a right ventricular infarction, are preload dependant ie., if we drop the preload, by giving a dilator such as GTN, they drop their blood pressure significantly. If you do give them GTN without looking at the Right Ventricular leads, they need IV fluid pushed, to improve the preload and they may need inotropes.
In a RIGHT VENTRICULAR INFARCTION the following are present on the ECG
- STE in III > STE in II and
- ST elevation in aVF > ST depression in V2.
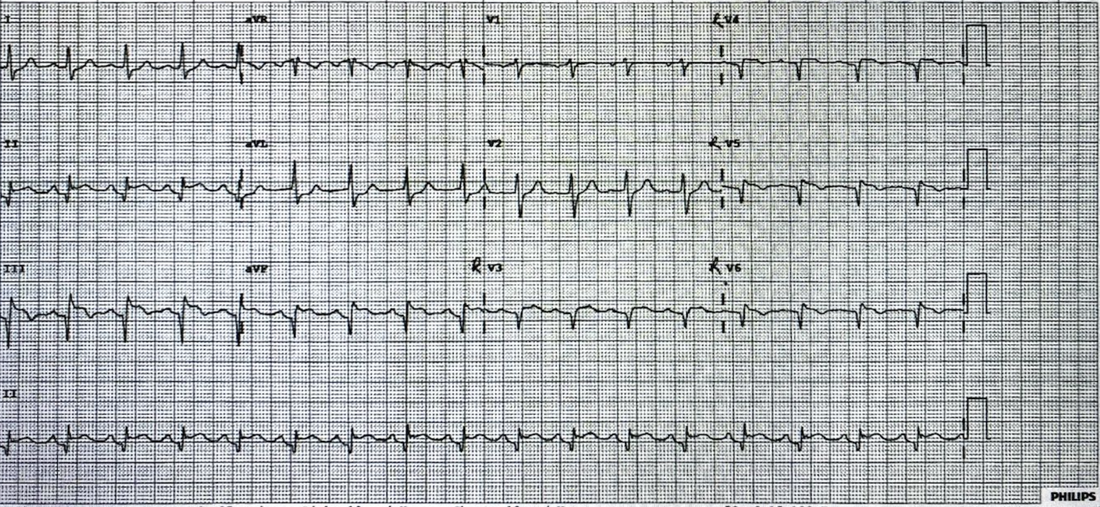
Right Ventricular leads were performed on this patient. See below. V4 is now right sided V4. RV4 is obtained by looking at the right side of the heart and placing V4 in the right mid-clavicular line in the 5th intercostal space.
ST elevation in RV4 has a 100% sensitivity and an 87% specificity and 92% predictive accuracy in diagnosing right ventricular myocardial Infarction.
BEWARE: In up to 50% of patients with a Right Ventricular Infarction the ST Elevation may disappear after about 12 hours. If there is no right ventricular ST elevation, but the patient decompensates following nitrates, suspect it.
What occurs in Right Ventricular Infarction?
With a right ventricular infarction, the right ventricle cannot pump properly and the right ventricular volume and end-diastolic pressure of the right ventricle are high. Due to the pump failure, the left ventricle is not receiving a sufficient amount of blood, but now the right ventricle with it’s increased volume also displaces the septum towards the left ventricle, decreasing its volume even further..
Anything that decreases preload ie., diuretics nitrates, beta blockers, morphine, can significantly decrease blood pressure. These patient may then require IV fluids and inotropic support.
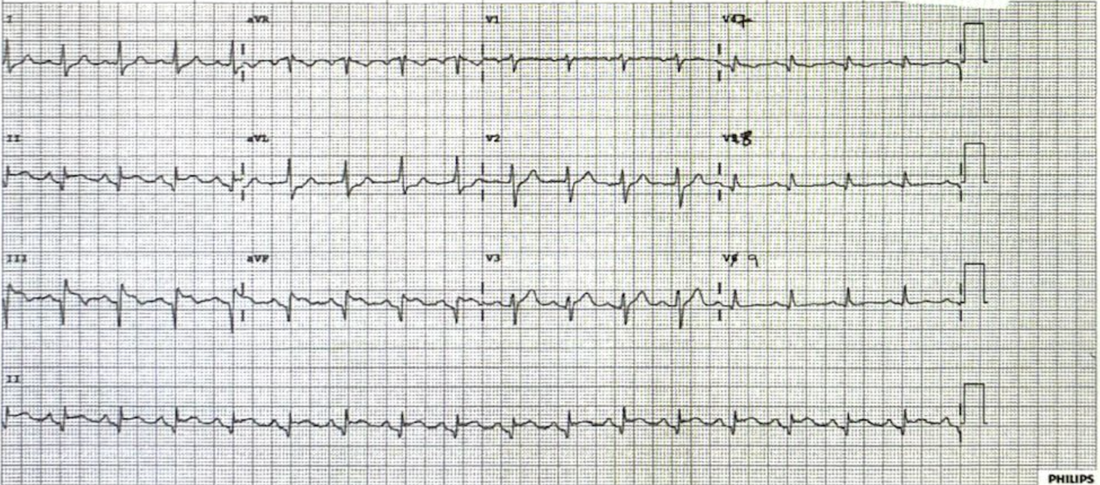
POSTERIOR Myocardial Infarction
Up to 20% of inferior infarctions will present as a posterior infarction. This represents a significantly larger area of infarction. The diagnosis is made by performing a posterior lead ECG ie leads V7-9. Some clues of a posterior infarction on the normal ECG include:
- Horizontal ST depression in V1-3
- Dominant R wave in V2
- Upright T waves.
The initial ECG showed some mild ST depression in V2, but little else. Posterior leads were performed, as shown in the ECG below.
OUTCOME
The patient was transferred out for catheterisation and diagnosis. A 100% right coronary artery occlusion was stented.
QUESTION: Could we have given thrombolytics?
Time from symptom onset, is a marker of downstream myocardial damage. Usually late presentations(>12 hours) are referred for percutaneous coronary intervention, although not always. Three studies (references given below) a worth reading here:
- The LATE Study: No mortality benefits using thrombolytics in those patients presenting > 12 hours
- BRAVE-2 Trial: Prognostic benefit in recanalisation in late presenters up to 48 hours.
- OAT Trial showed no improvement in mortality with PCI in very late presenters
My approach is that given that the patient was stable and had presented more than 14 hours following symptom onset, transfer for PCI was appropria
te. If there was no cath lab and there would be a significant delay in treatment, I would discuss thrombolysis with the Cardiologist. Rescue plasty could always occur later.
All Cardiac Bootcamp Self Study Course Members should review the topic ‘Subtle Ischaemic Changes’, in the syllabus, especially changes in aVL.
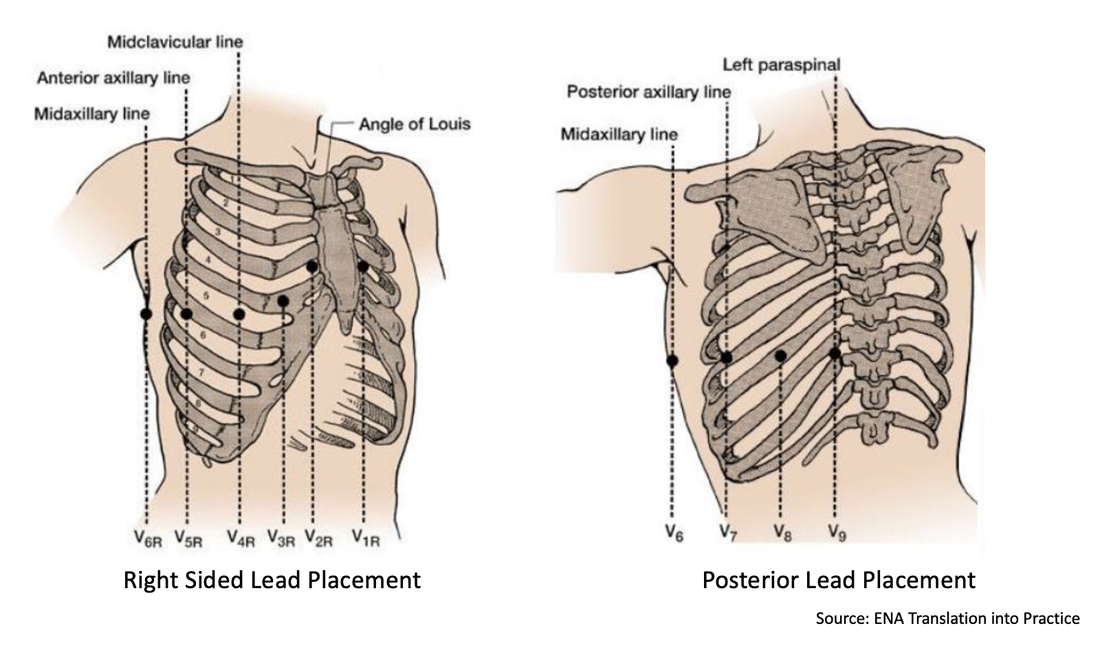
How to set up Right Sided and Posterior ECG Leads
- Hamon M, et al. Prognostic impact of right ventricular involvement in patients with acute myocardial infarction: meta-analysis. Crit Care Med. 2008 Jul;36(7):2023–33.
- Somers MP, Brady WJ, Bateman DC, Mattu A, Perron AD. Additional electrocardiographic leads in the ED chest pain patient: right ventricular and posterior leads. Am J Emerg Med. 2003 Nov;21(7):563–73.
- Shiraki H, Yokozuka H, Negishi K, et al. Acute impact of right ventricular infarction on early hemodynamic course after inferior myocardial infarction. Circ J. 2010 Jan;74(1):148–55.
- . Late Assessment of Thrombolytic Efficacy (LATE) study with alteplase 6–24 hours after onset of acute myocardial infarction. Lancet. 1993; 342:759–766.
- Ndrepepa G, et al. Mechanical reperfusion and long-term mortality in patients with acute myocardial infarction presenting 12 to 48 hours from onset of symptoms. JAMA. 2009; 301:487–488.
- Hochman JS, et al. Occluded Artery Trial Investigators. Coronary intervention for persistent occlusion after myocardial infarction. N Engl J Med. 2006; 355:2395–2407.








Great case and very good explanation regarding the leads placement and pathogenesis. Would you use Noradrenalin or anything else if BP drops due to inadvertent use of Gtn? Or just pump the fluids? Thank you