An elderly patient is brought into the ED with recurrent falls. There is a past history of Parkinson’s Disease.
The team is at handover and they see this wide complex tachycardia on the central monitor. The patient is not feeling very well. An ECG is done. What is the diagnosis? Below are some options for you to choose from.
What is your diagnosis? Pick one of the following:
(a) Ventricular Tachycardia
(b) Torsades de Points
(c) WPW with retrograde conduction
(d) Normal sinus rhythm with artifact
(e) Atrial Fibrillation with WPW
(f) Hyperkalaemia
…The answer is shown below…
When we look at a wide complex tachycardia there should be several differentials to entertain:
- Ventricular Tachycardia
- SVT with aberrancy
- Bundle Branch Block
- Hyperkalaemia
- Na channel blockade
- Ischaemia
- Paced rhythm
For members of the Cardiac Bootcamp Self Study Course, go to the section on wide complex rhythms and read all about how to make the diagnosis.
Here is my approach….
I apply the 120 CRAM rule to work out if it is VT. However before I do any of that, I look to see if this is a real ecg and not an impostor.
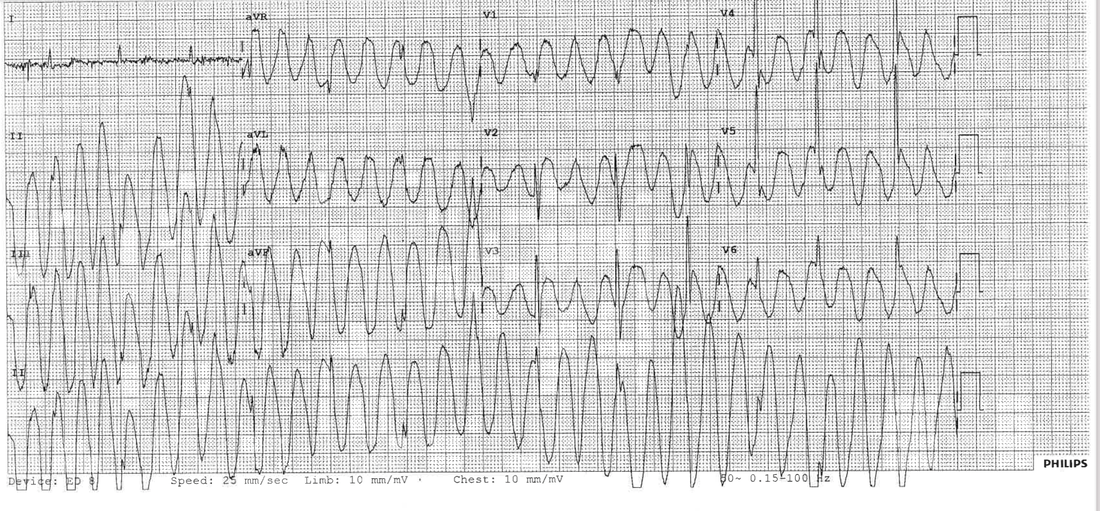
The ECG is wide complex and looks like VT, but is it real, or is it something else?
Let’s look at the ECG again. We can see that there is a definite underlying rhythm with an overlay of this wide complex.
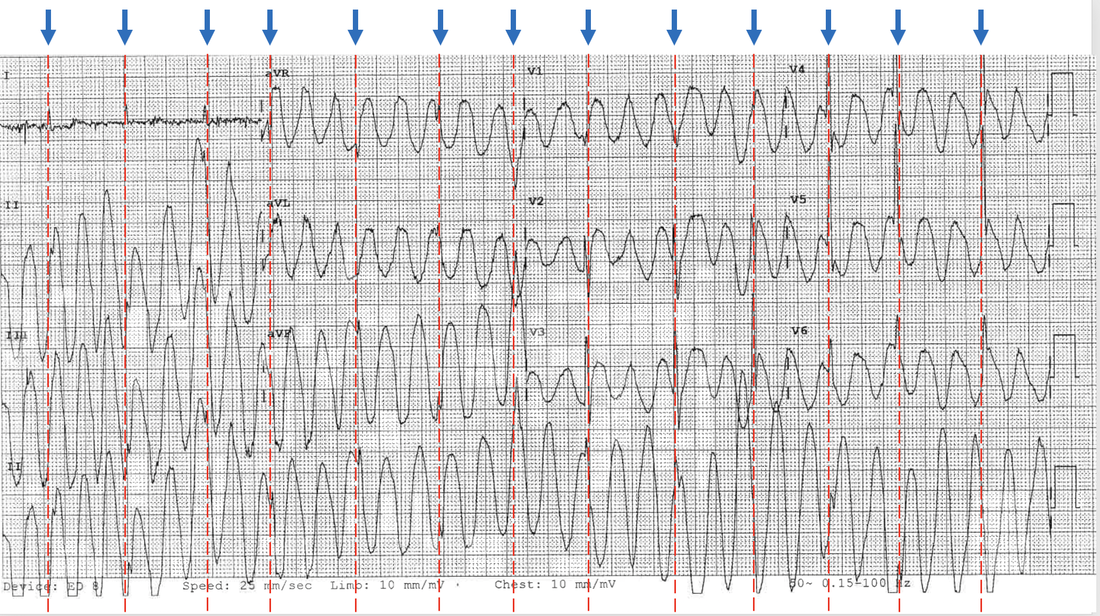
So this is a normal sinus rhythm with artifact. PLUS look at lead I. You can’t have every lead going into VT, but lead I refuses. “No I’m not doing it! I’m not going into VT”. So this is clearly a normal sinus rhythm with overlying artifact, which is probably related to the patient’s tremor secondary to their Parkinson’s Disease.
We can stop there. No need to apply the 120 CRAM formula. It’s an impersonator.
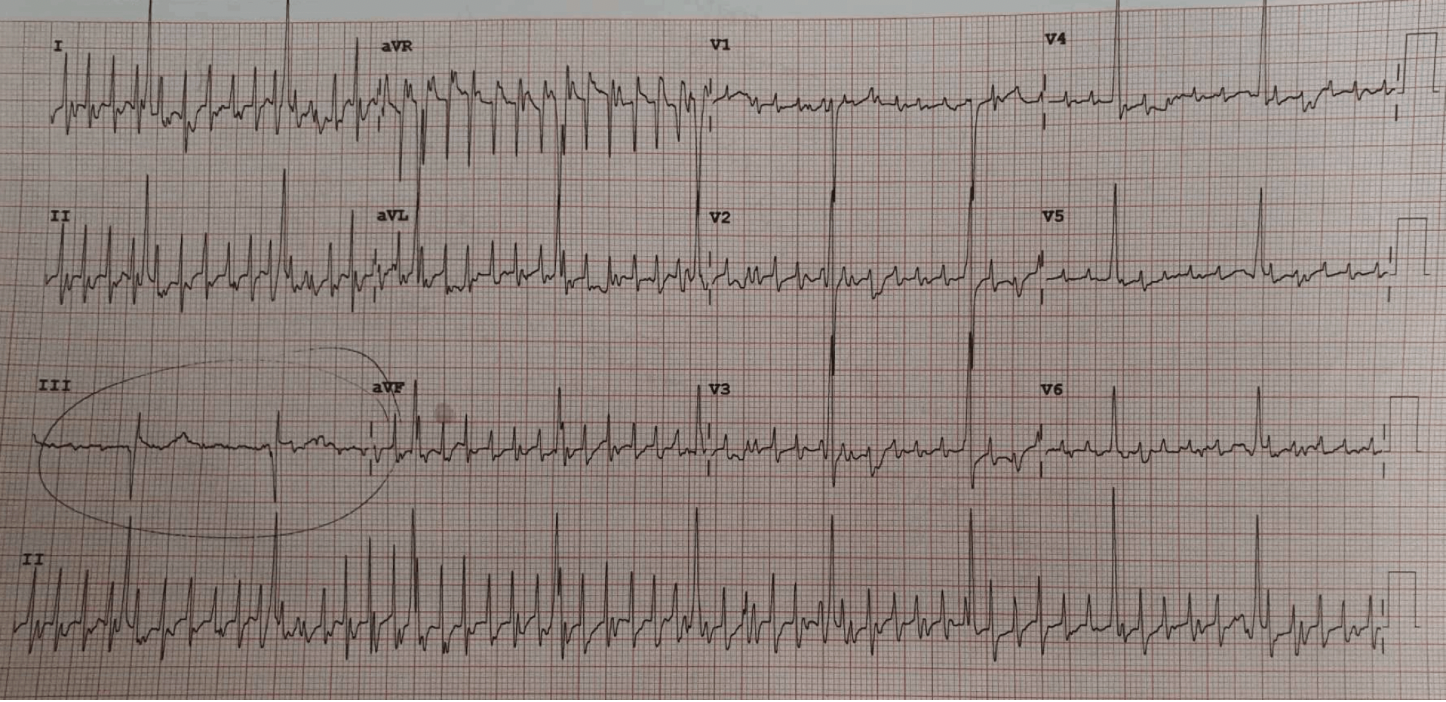
Below is another example, where a 35 yo male with cardiomyopathy presented with chest pain. The registrar made a diagnosis of atrial flutter based on the ECG below.
This is another impersonator rhythm. We see the patients actual underlying rhythm in lead III, all the rest of the leads show artifact. The patient had a tremor. Again, all the ECG leads can’t show atrial flutter but one lead ie., lead III refuses to go into flutter…stubborn. So it’s not real.
Think of this in the patient with tremor or with rigors etc., before you put the pads on.
Keep sending in those great ECGs. Thanks to Dr Einthoven.