An 82 yo patient is brought into the emergency department tachycardic, with a regular rate of 139 beats per minute and haemodynamically stable. She has a past history of atrial fibrillation for which she is on Sotalol. She is not anticoagulated at present, due to a previous intracranial bleed whilst on Apixaban.
According to the patient, she has recently had a viral chest infection, but has tested negative on swabs. She is afebrile and her GP has commenced doxycycline.
The patient is currently in a nursing home, although manages most of her ADLs with assistance. She was found to be tachycardic the evening before by nursing staff who supposedly performed a vagal manoevre with momentary effect, however the rapid current rhythm resumed.
The ambulance was called in the morning as the patient’s heart rate was still high. Vagal manoeuvres (REVERT), were performed, with momentary slowing of the rhythm, however this soon returned to its previous rapid rate.
An ECG taken on the patient’s arrival is shown below.
What does it show and what would you do next?
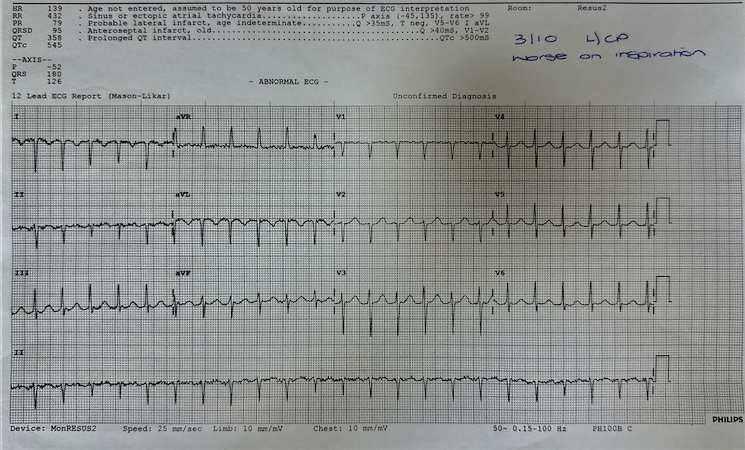
This looks like an SVT. However beware the ECG with a rate of 140 +/- 20, as it may be atrial flutter. I see this as being more common in patients with a previously history of atrial fibrillation.
The patient has a persistent cough, although no fever. A Chest X-ray is performed and shown below.
 The Chest Xray, shows some left basal consolidation and evidence of a ventriculoperitoneal shunt, which was placed during the episode of intracranial bleeding. The patients inflammatory markers come back very raised.
The Chest Xray, shows some left basal consolidation and evidence of a ventriculoperitoneal shunt, which was placed during the episode of intracranial bleeding. The patients inflammatory markers come back very raised.
Our working diagnosis is a chest infection given the x-ray, inflammatory markers and the pleuritic chest pain. The ECG may be SVT, although my suspicion is that this is atrial flutter.
We attempted a vagal manoevre in the emergency department with no result.
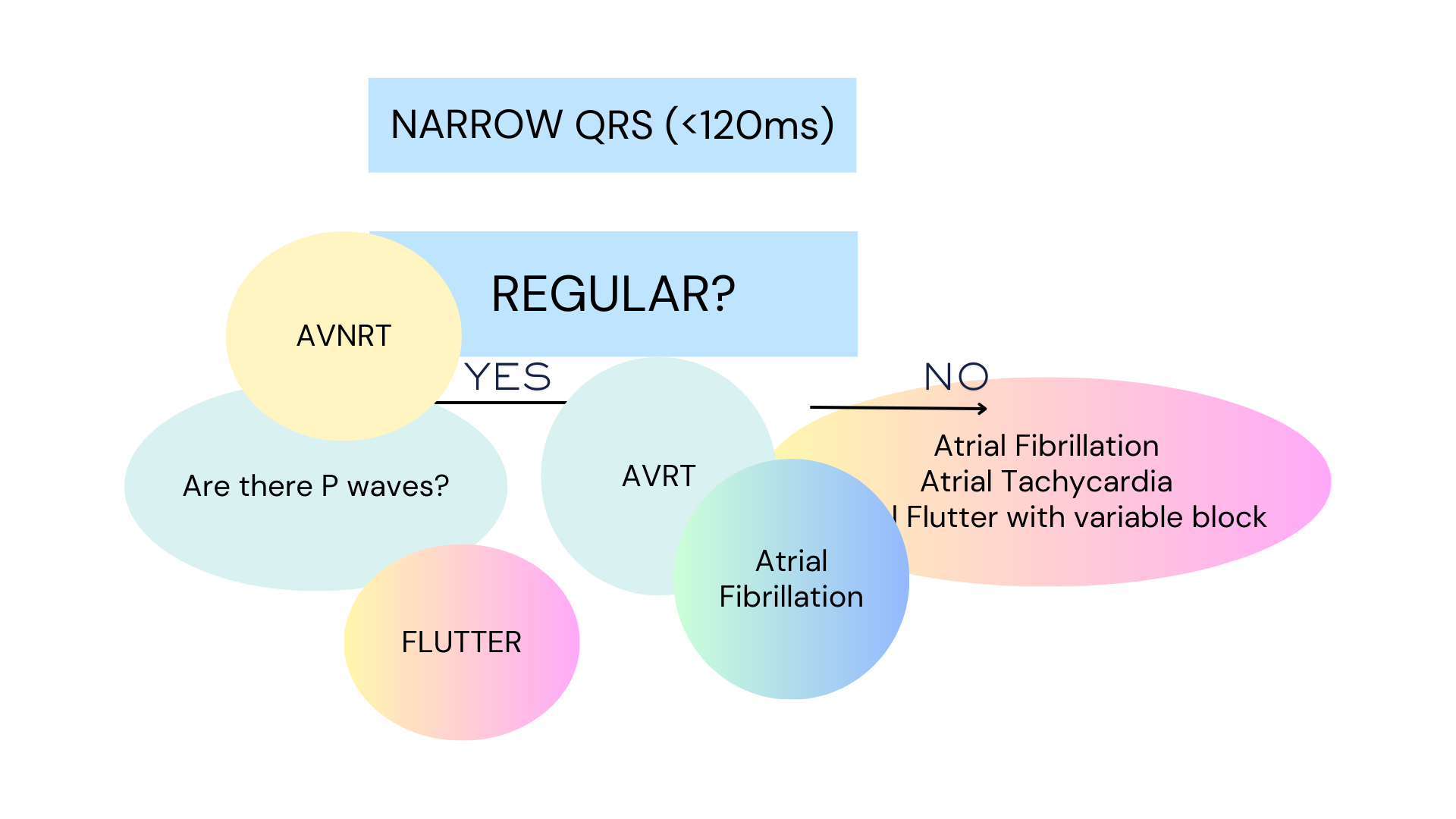
How do we make a diagnosis in suspected SVT?
Here are the steps to diagnosis, after establishing that it is narrow QRS is < 120ms:

1
- Is it regular?
- No? Then think of 4 diagnoses:
- Atrial Fibrillation
- Atrial Flutter with a variable block
- Atrial Tachycardia
- Multifocal atrial tachycardia
- Yes? Then think of the following.
- NO P waves visible: think AVNRT
- P waves are visible: is the atrial rate is > ventiricular rate
- If yes then suspect atrial flutter or atrial tachycardia
- If no think of:
- AVNRT
- AVRT
- Atrial Tachycardia
- No? Then think of 4 diagnoses:
Far more complex approaches can be used which includes the analysis or the RP interval and an evaluation of whether it is shorter or longer than the PR interval. However for simplicity the two steps shown above works well.
The Diagnosis
We believed that there were P waves seen, but not always.
Adenosine was given, and the AVN blockade exposed the underlying P waves. The rhythm strip is shown below:

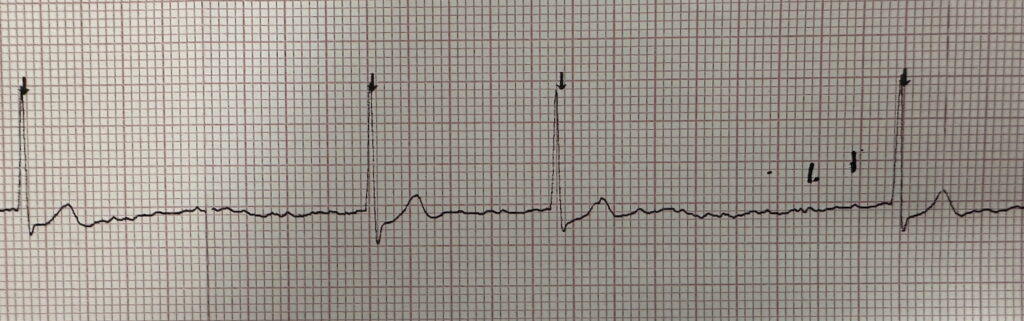
The diagnosis is Atrial Flutter.
What do we do now?
In this circumstance we would not rush in and cardiovert, unless the patient was unstable. We know that the likely cause of the flutter is the chest infection. Cardioverting a stable patient may result in the rhythm returning to flutter or reverting to atrial fibrillation, soon after the cardioversion is complete.
The approach is to treat the patient’s for the infection, with appropriate antibiotics. We will still need to slow the patient’s heart rate, as maintaining a rate of 139 beats per minute, will lead to ischaemia. Trying to reduce it to a normal rate is not approapriate as the tachycardia is due to the underlying infection and the compensatory effect of the tachycardia is of benefit to the patient.
The other consideration in this patient is that we want to slow the rate, without necessarily cardioverting the patient to sinus rhythm. Given that there is no anticoagulation here, cardioversion, may result in clot dislodgement and stroke.
What medications can we use to slow the heart rate?
- Beta Blockers: Like most other medications, this can lead to hypotension. There is a low chance of cardioversion, which may be an approapriate approach, given no anticoagulation. In many cases where patients have already been on a medication and are tolerating it well, it is approapriate to give them more of the same.
- Amiodarone: If there are no contraindications to this, amiodarone is an appropriate agent to slow the patients heart rate. It may also cardiovert the patient to sinus rhythm. In this case this may not be ideal.
- Calcium Channel Blockers: Like beta blockers, these are contraindicated in decompensated heart failure. If the patient has been previously on them, they may be considered.
- Digoxin: An old drug. It may actually help in heart failure as it does augment contractility. It also reduces heart rate.
Our patient was already on Sotalol (40mg BD), so an extra dose was given. Following this, the heart rate remained high. The patient was then loaded with digoxin and the heart rate soon dropped to 110 beats per minute.
Key Learning Points
- In any patient with a heart rate of 140 +/- 20, think of flutter, especially if there has been a previous history of atrial fibrillation.
- If difficult to diagnose, atrioventricular nodal blockade, may provide a window of opportunity to see the underlying P waves.
- Atrial flutter may be related to an underlying disease, such as sepsis. In these cases we treat the disease and not the flutter.
- Cardioversion, may be needed in the unstable patient. In all other patients treating the disease process and then trying to control the heart rate is the appropriate approach
- When lowering the heart rate, beware to not lower it to what is a ‘normal’ heart rate as tachycardia may be an appropriate compensatory response.







