
Video laryngoscopy (VL) versus Direct Laryngoscopy (DL). What should be the standard of care?
Yet another paper was published last month(1) looking at Video laryngoscopy (VL) versus Direct Laryngoscopy(DL). They found that for airways that were Cormack-Lehane > Grade 1 view, VL was superior to DL, especially for first pass success. The odds ratio was 3.14 in favour of VL! This is significant. The study was a little limited as it was a post hoc analysis and was not controlled, however it simply adds to the large body of evidence already out there.
The debate continues, but are we debating the wrong thing? The concern appears to be that if VL were the only technique learnt, it would lead to a degradation of skills with DL. What happens if all we train in is VL but for some reason it is unavailable?
My concern is that this is the question we are asking. What we need to be asking is what is the best technique that I can use….AND what is my backup plan? We need to be proficient in two techniques. The second technique for me is DL
In a Cochrane Review published in 2022 (2), they found that VL:
- Improved intubation success rates especially in difficult airways
- Reduced the number of failed attempts
- Improved glottic view and reduced the chance of airway trauma
A recent Pro-Con debate(3) amongst anaesthetists, on whether VL should be the standard of care for intubations addressed many of the current concerns around the topic.
Aziz (3) discusses the term standard of care and the fact that it has legal implications and can be associated with negligence and liability, so it may be important to not designate that title to VL, but consider it as a very important procedure.
The need to use the best technique available is similar to using ultrasound to pass a central venous line(3). If we don’t use landmarks to place a central line but use ultrasound, are we at risk of losing those skills? If so we shouldn’t use ultrasound. We know this argument is flawed. The answer is to know how to use both techniques.
VL doesn’t have a 100% success rate. Very few techniques do. It does not perform any better than DL, in those cases where the view was adequate (4), or in cases where more than one attempt at intubation occurs (2). VL may lead to a longer time to successful intubation, which can be important in time critical intubations and may result in worst outcomes in trauma patients (5).
My approach is that VL is my first choice for intubation. We must assume that most of the airway cases we deal with in the emergency department are difficult airways. Knowing that predicting difficult airways is diffciult, it makes sense to use this. I also believe that we need to be proficient in a second technique. We must always have a fallback plan.
The second technique for me, will not necessarily be a hyperangulated blade VL, as this requires new technique. It will be DL. For that reason when using VL, I insist on a standard Mac blade architecture, as I use in DL. I teach both and alternate between the two. Should it be standard of care? I believe so, however that term has legal connotations associated with it. I approach it the same way as I approach using an ultrasound for central line placement…..it is my preferred technique.
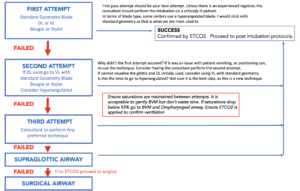
Below is my approach to the Airway. I will speak more about this at EMCORE.
References
- Prekker M E et al. Laryngoscopy and Tracheal Intubation: Does Use of a Video Laryngoscope Facilitate Both Steps of the Procedure? Ann Emerg Med 2023 Apr 5;S0196-0644(23)00126-9. doi: 10.1016/j.annemergmed.2023.02.016. Online ahead of print.
- Hansel J, et al. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst Rev. 2022;4:CD011136.
- Aziz M F et al Pro-Con Debate: Videolaryngoscopy Should Be Standard of Care for Tracheal Intubation. Anesthesia & Analgesia April 2023 136 (4): pp 683-688
- Aziz MF, et al. Comparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airway. Anesthesiology. 2012;116:629–636.
- Yeatts DJ, et al. Effect of video laryngoscopy on trauma patient survival: a randomized controlled trial. J Trauma Acute Care Surg. 2013;75:212–219.







