
HOT OFF THE PRESS: A new clinical trial showing that rapid IV fluid administration does not affect neurological outcome in children with DKA, as has previously been thought.
Clinical Trial of Fluid Infusion Rates for Pediatric Diabetic Ketoacidosis. N Engl J Med 2018; 378:2275-2287
The Numbers
This was a randomised controlled trial in 13 centres. 1255 children were enrolled with 1361 episodes of DKA, which was defined as:
- pH < 7.25 or
- HCO3 of <15mmol/L
Most of the evidence we have thus far is retrospective and implies that a rapid infusion of fluids decreases serum osmolality, resulting in brain swelling. Slow rehydration has been advocated. This study challenges that and shows that other mechanisms are at play.
What They Did
This study compared rapid fluid administration and slow fluid administration using 0.45% Saline and 0.9% saline in the following way.
- The FAST FLUID ADMINISTRATION GROUP was assumed to have a 10% body weight fluid deficit.
- These patients received 10mL/kg fluid bolus and a second 10mL/kg bolus
- Half the deficit plus maintenance was replaced over 12 hours and the other half over 24 hours
- The SLOW FLUID ADMINISTRATION GROUP was assumed to have a 5% body weight fluid deficit.
- These patients received 10mL/kg fluid bolus, but no second bolus
- Maintenance and deficit were replaced over 48 hours
PRIMARY OUTCOME
This was a deterioration in GCS < 14: measured as two consecutive scores of GCS<14 in the first 24 hours.
SECONDARY OUTCOMES
These were memory impairment and apparent brain injury resulting in hyperosmolar treatment or intubation.
RESULTS
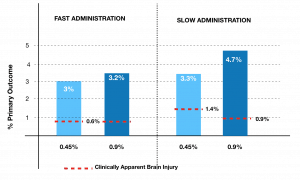
The above graph shows that patients with slow administration of fluids had an increased frequency of ‘primary outcome’ (GCS<14) ie., they did worst. Those patients with rapid IV fluid administration had a lower rate of clinically apparent brain injury. These are trends however, as there was no statistically significant difference between the two groups.
DISCUSSION
An interesting paper with some minor limitations, that however challenges the notion that rapid infusion of fluids leads to worst outcomes.
ADDITIONAL COMMENT
The issue of late fluid volumes has been a concern in the past and this study does address that….sort of. One group received 20mL/kg and assumed 10% dehydration and the other received 10mL/kg and assumed 5% dehydration.
This may be a practice changer. Will this change your practice?
It probably won’t change mine at the moment, nor quite a few people that have responded, to this blog, but a gutsy study. If the child needs fluid resuscitation, give it to them, (5-10mL/kg and repeat if have to). If they don’t, go slow. The previous evidence has shown significant issues with volumes of over 40mL/kg. I’m not sure that such volumes are needed.
You may also want to read 2 other blogs written on the topic:







