What does Upward Arm Drift mean?
A 50 yo patient presents to the emergency department complaining of difficulty holding things with the right hand for the past 5 days. An important sign found on clinical examination is shown in the video below.
What is the sign shown? Where is the lesion?
Read the case and find out all about it.
The Case
A 50 yo patient presents with right hand weakness for 5 days. Initially, the patient experienced numbness in the right hand and had difficulty performing fine movements, as well as holding and handling objects with that hand. There were no other symptoms.
The patient attended their General Practitioner three days later as the symptoms were continuing. A CT brain was done. The patient was then contacted by the reporting radiologist, 2 days after this, and was told there there was evidence of a stroke and that they should present to the emergency department. The CT report was sent by text to the patient.
On Examination
The patient was well, with no past medical history and was on no regular medications.
Vitals were essentially normal, except for a tachycardia of 120bpm, which was related to anxiety following reading the CT report(it contained the differential of a tumour). This tachycardia settled quickly, following an explanation of what differentials were and a discussion.
A rapid neurological examination was conducted.
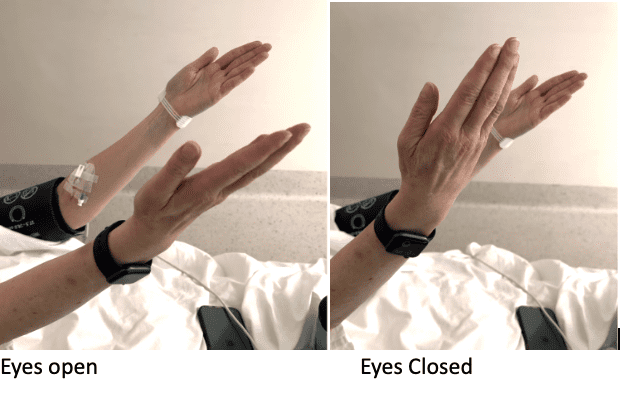
- Pronator drift was tested with the patient’s eyes open and then closed. With the eyes open, there was minimal pronator drift. With the eyes closed, there was a definite upward drift of the right arm, as shown in the video. The upward drift found, was consistent with a contralateral parietal lesion, ie., a left middle cerebral infarct. This infarct was demonstrated in the CT brain.
- Forearm rolling and fine motor movements of the fingers were abnormal.
- Grip strength and finger abduction of the right hand was significantly reduced.
- There was also a global sensory impairment of the right arm.
- The cerebellar examination was normal.
- The was no visual neglect.
UPPER LIMB SIGNS TO LOOK FOR
It has been found that the best combination of neurological tests/signs for potential subtle pyramidal weakness are:
- Pronator Drift Sign
- Finger Tap Sign
- Deep Tendon Reflexes
If all three tests are abnormal, there is a specificity of 97.5% and positive predictive value of 94.2% for a stroke(1).
Pronator Drift Sign

The pronator drift sign can detect subtle upper motor neuron lesions.
The patient sits with their arms extended in front of them, elbows straight and palms facing upwards. They need to hold this position for 30 seconds.
The normal response is no change, a slight deviation bilaterally, or a slight pronation of the dominant hand.
An abnormal response includes the following:
- Downward Pronator drift with eyes open. The affected side, which is contralateral to the lesion, will drift downwards with pronation, as the pronators are more powerful than the supinators. This indicates a motor deficit and a contralateral middle cerebral artery territory stroke. Please note that a downward drift of the arm without pronation is considered to be potentially functional in origin.
- Downward pronator drift with eyes closed. This demonstrates that position sense is affected and indicates a posterior column lesion. It may also indicate neglect.
- Upward arm drift with eyes closed. This indicates a loss of position sense and is usually caused by a contralateral parietal lesion.
- Upward and Outward drift with eyes closed. This indicates a cerebellar drift.
Here is a demonstration of the above at a recent EMCORE Conference.
Finger/Forearm Rolling Test
The patient is asked to roll the index fingers or the forearms around each other, in each direction for a few seconds. If there is weakness, the normal arm rotates around the abnormal arm ‘like a satellite’.
The Mingazzini Sign(3)
 Mingazzini was an Italian Neurologist, who in 1913 introduced this sign to detect subtle weakness. The patient holds their arms straight in front of them, with their fingers spread, for as long as possible. The test is considered positive when one wrist or arm starts to drop, or the fingers cannot be maintained in abduction. In an upper motor neuron lesion, the hand should be affected before the arm is affected.
Mingazzini was an Italian Neurologist, who in 1913 introduced this sign to detect subtle weakness. The patient holds their arms straight in front of them, with their fingers spread, for as long as possible. The test is considered positive when one wrist or arm starts to drop, or the fingers cannot be maintained in abduction. In an upper motor neuron lesion, the hand should be affected before the arm is affected.
A similar test was also proposed for the lower limb. The patient lies on their back, with legs raised at right angles to the trunk and the knee bent at 90 degrees. The lower limb must be kept horizontal. Weakness will result in the lower leg not being able to maintain that horizontal position.
Fine Finger Movements
The patient taps the thumb and index finger of the same hand together, rapidly, several times. A pyramidal lesion may decrease the amplitude of the motion, on the contralateral side. A cerebellar lesion will result in irregular and varying movements.
Deep Tendon reflexes
Abnormal reflexes are defined as an increase in reflexes on one side, or the presence of a positive Babinski reflex(stimulation of the lateral plantar aspect of the foot, resulting in dorsiflexion of the great toe).
Conclusion
The neurological examination is an important part of our clinical assessment of the patient who presents with weakness or a sensory deficit. We don’t need to initially conduct an extensive neurological examination in the emergency department. A simple approach, such as that shown above, for the upper limb examination, using signs that can detect subtle changes, allows us to rapidly make a diagnosis.
References
- Teitelbaum J et al. Tests of motor function in patients suspected of having Mild unilateral cerebellar lesions. Can J Neurol Science 2002;29:337-344
- Sawyer RN et al. Asymmetry of forearm rolling as a sign of unilateral cerebral dysfunction. Neurology 1993; 43:1596-1598.
- Mingazzini G. Sur quelques “petits signes” des paresies organiques. Revue Neurologique. 1913; 20(2): 469-473







