
This week I have 4 questions for you. 3 are ECGs you must know and the fourth is a simple question on what you should look for in the QRS complex, when reading the ECG. Enjoy. Hope to see you at the Live Cardiac Bootcamp Course on the Gold Coast in January 2022. Congratulations to everyone who has purchased the Online Cardiac Course and thank you for all the great comments. New sections added regularly..
ECG 1
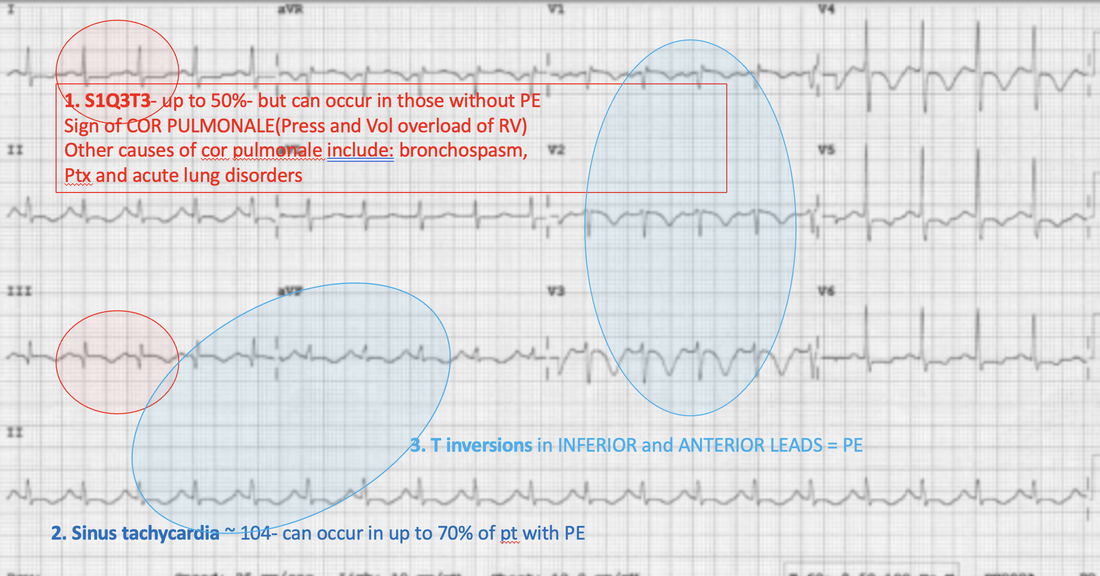
A 69 year old woman presents with dyspnoea. Her ECG is shown below. Describe the ECG and interpret the changes by giving your most likely diagnosis.

Perm J. 2011 Fall; 15(4): 75.
ANSWER
The diagnosis is most likely a pulmonary embolism. There are 3 main ECG changes seen on this ECG.
ECG 2
In my ECG in 20 seconds method, what are the 4 things to look for when looking at the QRS?
ANSWER
- Are they TALL or are they small?
When looking at the QRS complex look to see if there is any evidence of hypertrophy. The Sokolow-Lyon method is the one I use. It allows rapid reading. I add the amplitudes of the S wave of V1 to the R wave or V5 or to V6.
Are the QRS complexes small? ie., is there something between them and the reading electrodes? This may be fluid or fat. Pericardial or pleural effusions are the ones to consider. Small complexes and tachycardia, should always make us think of a pericardial effusion. - Are they Wide or narrow?
Here I am looking to see what the cause of a wide complex is. Sometimes we couple this question with fast or slow. For example, slow rates with a wide complex may be associated with a complex being initiated outside the atrioventricular node. If a complex passes through the AV node, it is narrow. Wide complex fast rhythms may be due to a number of causes including ventricular tachycardia, hyperkalaemia, Na channel blockade, ischaemia and more. - Do they have abnormal morphology?
This is really referring to the delta wave of WPW - Are they clumped?
This is a step I have included to ensure we don’t miss a Moritz block( which we would normally look for in the previous step). In mobitz blocks, we often (not always) see a clumping of the QRS waveforms. This reminds us to go back and look for a Moritz Block more closely.
ECG 3
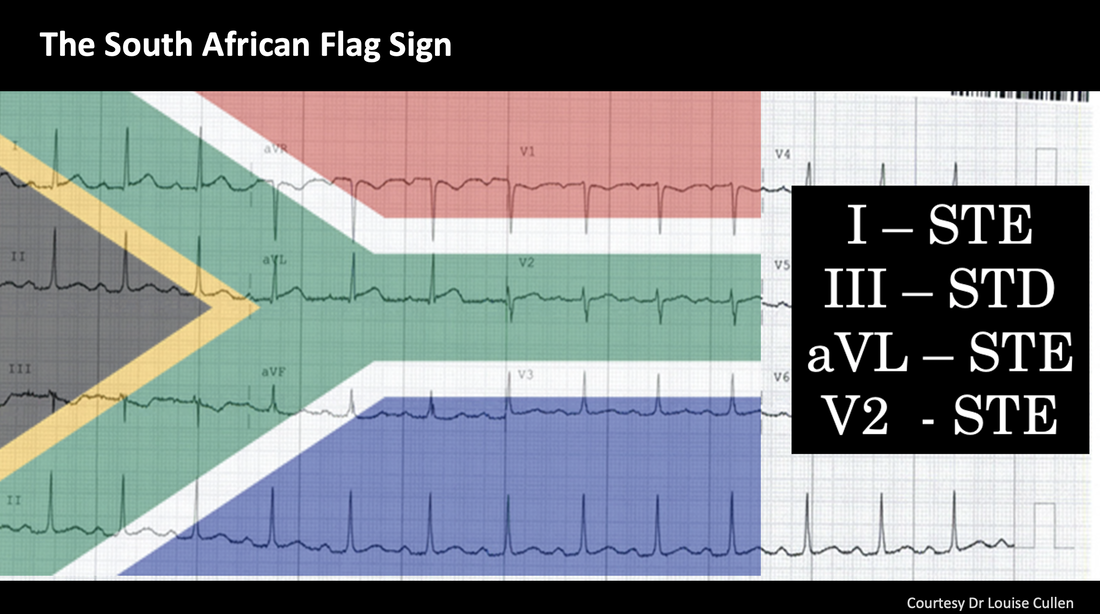
A 54 yo male presents with chest pain, that radiates into his jaw. He has a previous history of an AMI 10 years previously and also has hypertension, diabetes and hypercholesterolaemia. An ECG is done. Does this patient need to go to the Cath lab? What is the ‘sign’ seen here?
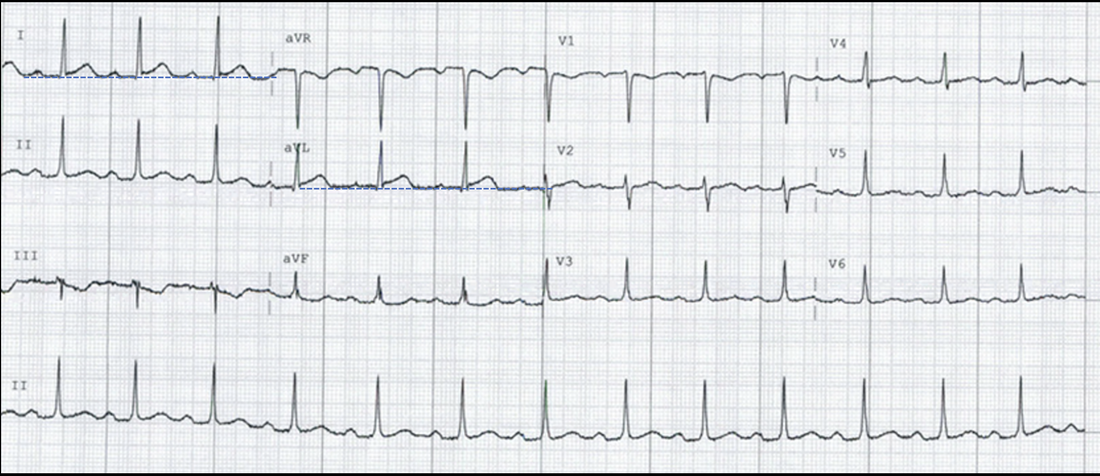
Image courtesy of Dr Louise Cullen.
ANSWER
This is a’The South African Flag Sign’. The patient had an obstructed diagonal artery.
ECG 4
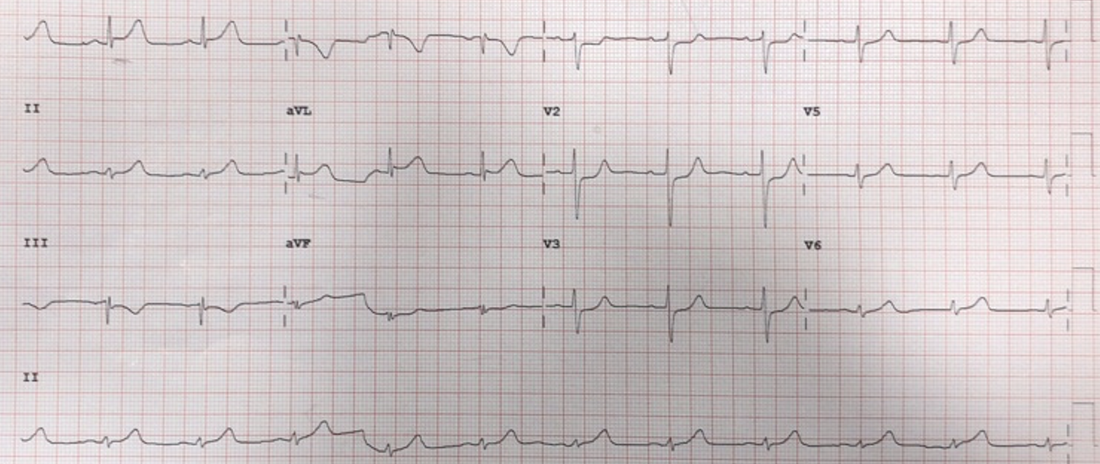
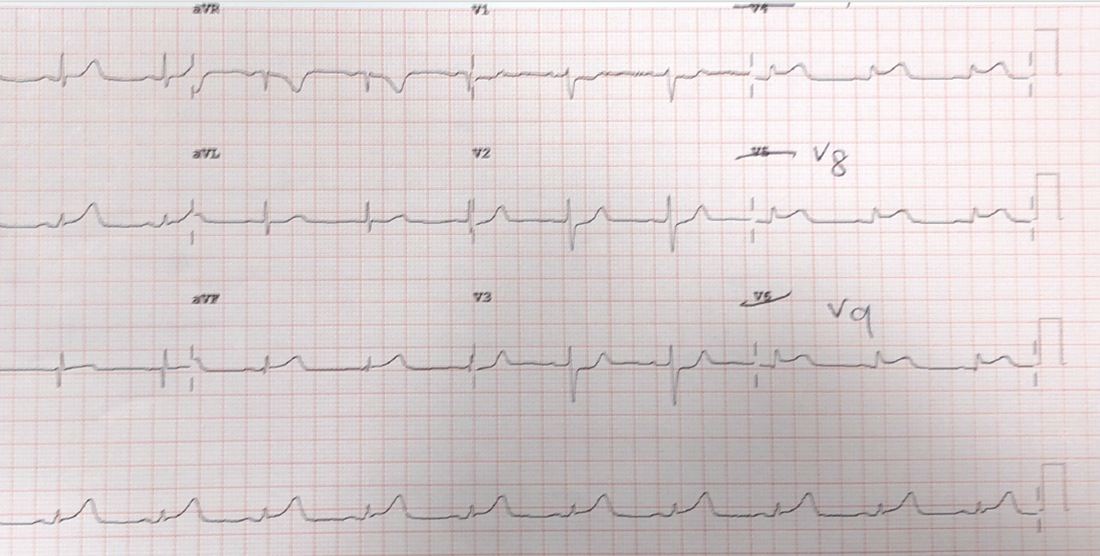
A 64 yo male presents with chest pain. What are the important ECG changes and what other ECGs would you perform?
ANSWER
The ECG shows ST depression in leads V1-V3. The anterior leads show reciprocal ecg changes, as no leads look directly at the posterior part of the heart.
Posterior leads are done here and the ECG is shown below. This is another STEMI Equivalent. This patient needs to go to the Cath lab.
Posterior leads are done here and the ECG is shown below. This is another STEMI Equivalent. This patient needs to go to the Cath lab.








Hi Peter,
Thank you very much for your very practical and educational approach to our daily work issues.
As somebody who is still deep in the trenches of Emergency Medicine, I enjoy reading your EM stuff as there are a lot of words of wisdom in what you present.
Keep doing good work
Regards from always rainy Ireland