Difficult ECGs
CASE 1
A 30 yo male presents to the emergency department with intermittent palpitations. The palpitations are are associated with a few episodes of depressed conscious state lasting a few seconds. He states he feels a little dizzy, however his blood pressure is 128/65. His ECG is shown below.
What is the diagnosis and how would you treat the patient?

What does the ECG show?
This is Torsades de Pointes (Twisting of the Points). It is a form of Polymormic VT associated with prolonged QT. The twisting of the points is the result of the QRS axis changing.
In this case, the patient was on Methadone, known to prolong QTc.
How would you treat this patient?
Your first option is to offer the patient electrical cardioversion. This would be very appropriate, however the patient is continuing to go in and out of this Torsades Rhythm. and refuses electrical cardioversion. What medications would you offer?
Could you give Amiodarone?
No. Amiodarone like Procainaimide prolongs QTc and although it may be used as treatment of monomorphic VT, it may make things worse here.
We should not use Amiodarone and Procainaimide.
What is the treatment of choice?
We can use any of the following:
- Magnesium Sulphate
- Isoprenaline
- Pacing
- Lignocaine
CASE 2
A 30 yo patient presents to the emergency department, with a complaint of palpitations. The patient is well looking and haemodynamically stable.
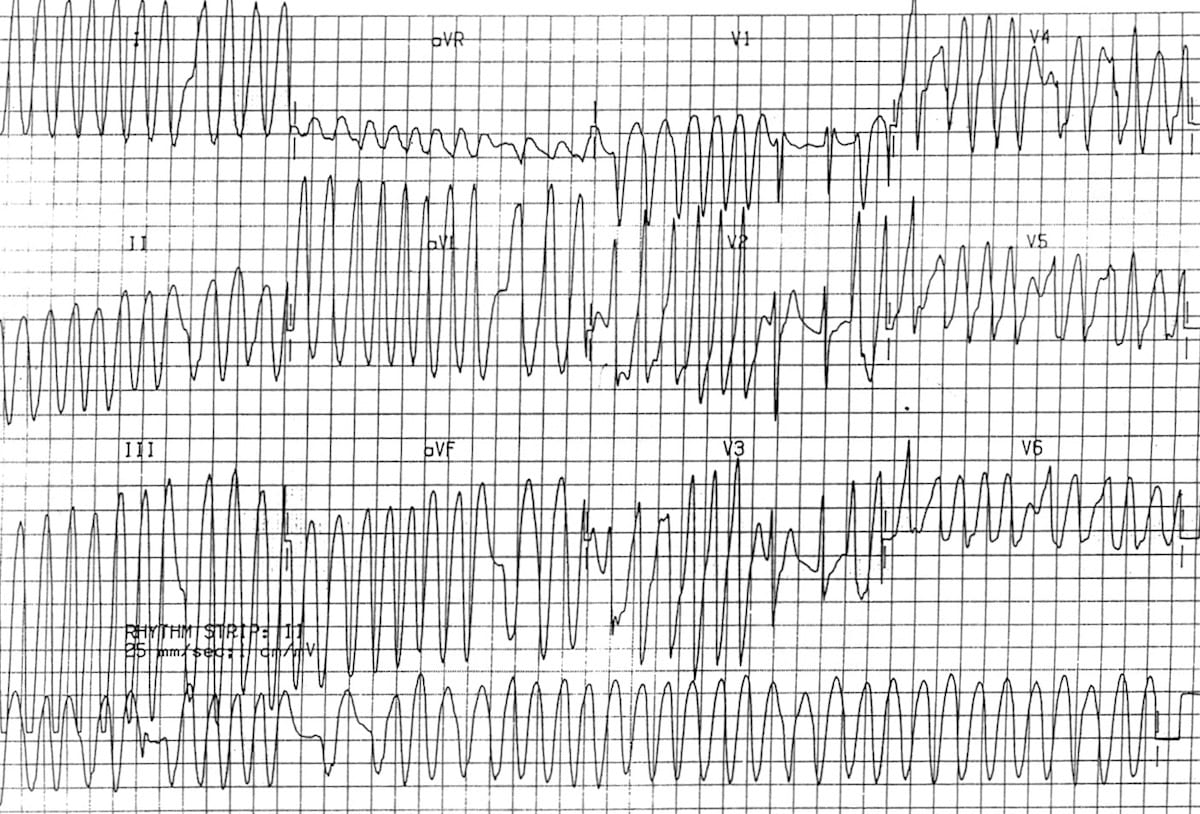
The ECG is shown below. What does it show?
What is your diagnosis?
You offer the patient cardioversion, but they refuse.
What will you use to medically cardiovert this patient? Pick one.
(a) Magnesium
(b) Amiodarone
(c) Procainaimide
(d) Metoprolol/Esmolol
Answer
The diagnosis is AF with WPW.
This means that there are complexes conducted through the AV node and also through the accessory pathway, making some complexes narrow and some wide. It is irregularly irregular.
The rate is the key. What is the fastest rate here? In some places the rate appears to be >300 bpm, although this is not sustained.. Whenever we see a rate that is > 220-250 bpm in an adult, there must be an accessory pathway in exitence. In children, there are accessory pathways present in the very young, which disappear later in life.
In an adult we have to assume that there is an accessory pathway when the rate is that high. Therefore it must be WPW. It is also irregularly irregular so is AF with WPW.
If we give anything that blocks the AV node, all the complexes will be conducted down the accessory pathway. The ventricle can’t support rates of 300 bpm or more, for any prolonged period and so will begin to fibrillate. The rhythm will now be Ventricular Fibrillation and the patient is in cardiac arrest.
Procainaimide is the only drug in this group that blocks the accessory pathway preferentially, so is the treatment of choice here.
How do we differentiate Torsades de Pointes from AF with WPW?

The QRS axis changes, ie., the QRS’s point in different directions.

In AF with WPW, the QRS’s all point in one direction.

To be an expert at Emergency Medicine Cardiology: Join us at a LIVE Cardiac Bootcamp. Or get the 12 month subscription to the online course.