
Below are 2 cases we have all been confronted with, in the Emergency Department. Which medication is best to support the blood pressure in each case?
Case 1
A 68 yo male is brought to your emergency department in what appears to be septic shock. He has had a recent urine infection. Over the last 24 hours he has become quite febrile and lethargic according to his wife. This morning he felt unwell and felt like he was going to collapse each time he tried to get out of bed.
On arrival he is alert and oriented. He feels unwell. His vitals are as follows:
- Temperature 38.9
- Heart Rate 115 bpm
- Blood Pressure 78/46
- Sats 96% on room air.
The ambulance have given him one litre of Normal Saline and he is on his second Litre.
You make the diagnosis of Septic Shock most likely due to urinary cause and immediately give antibiotics. The second litre of fluids is now in. (In fact, a gram stain result comes through in the next few hours with a G-ve bacillus)
What do you give next? Here are some choices:
- Adrenaline
- Noradrenaline
- Dopamine
- Isoprenaline
- Dobutamine
- Milrinone
- Vassopressin
We’ll come back to this case in a minute.
Case 2
A 65 yo male is brought in by ambulance. He has had chest pain for the previous 3 hours. He is diaphoretic and looks unwell. His BP is 71/50 and he is speaking in single words, with saturations of 90% on a non-rebreather. His chest examination has widespread crepitations.
He has no relevant past medical history.
Hi ECG is shown below:
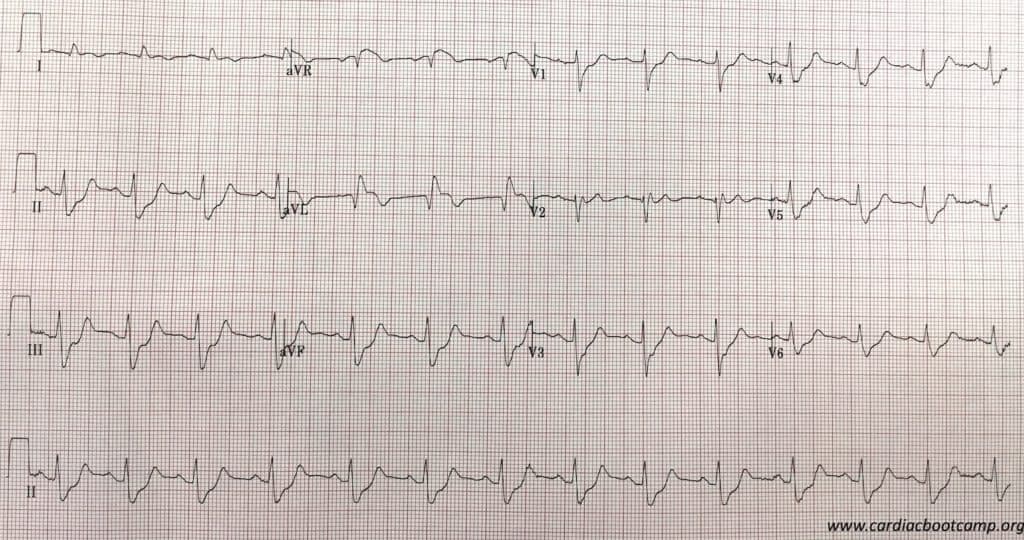
You diagnose a probable LAD occlusion and that the patient is in cardiogenic shock. Your hospital doesn’t have a Cath lab and so you decide to thrombolyse. However, you also need to sort out the cardiac failure and the blood pressure.
GTN is not an option to dilate due to the cariogenic shock. You decide on CPAP for the breathing but need to support the blood pressure. What do you use?
- Adrenaline
- Noradrenaline
- Dopamine
- Isoprenaline
- Dobutamine
- Milrinone
- Vassopressin
We’ll come back to this case in a minute.
What are we trying to achieve in shock?
Below is an image I put up at each of our face to face cardiac bootcamps and in the Cardiac Bootcamp Online Course.
We are trying to increase the Mean Arterial Pressure(MAP).
MAP = (SBP + (2xDBP))/3
From this equation we see that the diastolic blood pressure is a very important part of the MAP. Quite rightly so, as the diastolic pressure relates to cardiac filling and coronary perfusion.
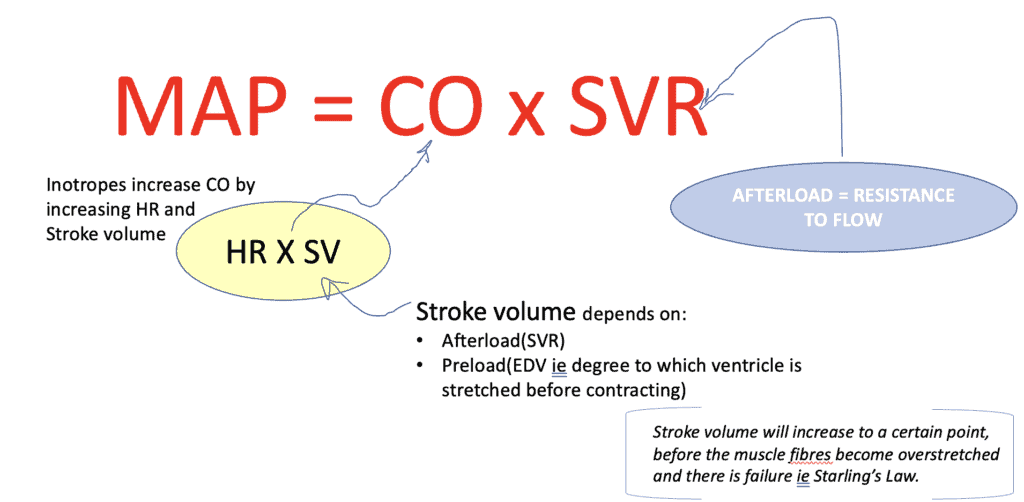
It’s all a careful balance. It’s not about just flogging the heart. We must also pay attention to how much blood goes into the heart and the pressure against which the heart is trying to pump that blood out.
The Cardiac Output is determined by the stroke volume and the heart rate. The Preload and Afterload play a very significant part in this. Is there enough preload that the heart fills and is the Afterload so high that the heart cannot pump against it? There’s more to think about that just stick up an infusion.
Preload and Afterload
PRELOAD: Think of this as reflecting the volume status. It increases with hypervolaemia and decreases with hypovolaemia. It is the ventricular stretch at the end of diastole.
AFTERLOAD: It is the resistance that the Left Ventricle must push against to circulate blood. The higher the afterload, they greater the myocardial work needed and thus the greater the oxygen demand which results in a decreased cardiac output.
Afterload Increases with:
- Vasoconstriction
- Aortic Stenosis
- LV Dilatation
- Hypertension.
What is the difference between a Vasopressor and an Inotrope?
A Vasopressor increases systemic vascular resistance and an Inotrope increases cardiac contractility
There is a third property we may require: Vasodilation.
Actions of medications and their use.
Please note that I will not be discussing Dopamine as part of these.
AT A GLANCE
α1 = vascular(arterial) smooth muscle
β1 = Heart: Increases rate and force of contraction
β2 = Bronchial Smooth muscle dilatation
| DRUGS | WHEN TO USE | RECEPTORS |
| ADRENALINE | Cardiac Arrest Anaphylaxis Shock (cardiac/vasodilatory) Bronchospasm Bradycardia |
ααααα β1β1β1β1β1 β2β2β2 |
| NORADRENALINE | Shock (cardiac/vasodilatory) | ααααα β1β1β1 β2β2 |
| DOBUTAMINE | Low cardiac output: -heart failure -cardiogenic shock -sepsis leading to myocardial dysfunction |
α β1β1β1β1β1 β2β2β2 |
| MILRINONE | Low cardiac output states in heart failure | cAMP |
| ISOPRENALINE | Bradycardias | β1β1β1β1β1 β2β2β2β2β2 |
| VASOPRESSIN | Shock (cardiac and vasodilatory) cardiac arrest. |
INOPRESSORS: Adrenaline and NorAdrenaline
Adrenaline (αβββ)
Non-selective adrenergic agonist: acts on α and β receptors. At low doses, acts on β2 receptors causing vasodilation. At higher doses its effect on α1 and β1, resulting in positive inotropy and vasoconstriction( of peripheral vasculature and pulmonary arterial and venous circulation).
It is both a chronotrope and an inotrope
It’s use is mostly in anaphylaxis and cardiac arrest as other drug combinations have been found to be better for both septic and cariogenic shock.
NorAdrenaline (αααβ)
It acts on vascular α1 adrenergic receptors, causing vasoconstriction and thus increasing systolic and diastolic blood pressures. It has chronotropic and inotropic effects by acting on on cardiac α1 receptors.
It can cause tachycardia and increase myocardial oxygen demand. It may also have a direct toxic effect on cardiac cells. It is the first line management of septic shock and may be used with other medications.
INODILATORS: Dobutamine and Milrinone
Dobutamine (αββ)
Dobutamine, a synthetic catecholamine, acts on β1 receptors increasing cardiac contractility. It also has α1 and β1 effects on peripheral vasculature resulting in vasodilatation at lower doses, thus increasing cardiac output. At doses above 5mcg/kg/min it can result in vasoconstriction.
It is usually used with an inopressor in cariogenic shock.
A meta-analysis, showed Dobutamine to be associated with higher in-hospital mortality and readmission rates for heart failure exacerbation when compared to nesiritide therapy. Higher doses of dobutamine is not preferred in patients with recent myocardial ischemia, as it can increase myocardial oxygen demand and induce tachycardia.
Milrinone
It is a Phosphodiesterase Type 3 inhibitor(PDE3) used inotropic agent in patients with cardiogenic shock. It inhibits PDE3, which results in more calcium ions entering the myocardial cell, increasing cardiac contractility. It also acts on peripheral and pulmonary vasculature leading to vasodilatation as well as inotropic effect. It does not act on the beta adrenergic pathway.
Another feature of the mechanism of action of milrinone is that the same intracellular processes is activated in smooth muscle cells of the peripheral and pulmonary vasculature, leading to a net vasodilatory effect in addition to its positive inotropic effect.
In a sub-group analysis of the OPTIME-CHF trial, it was found to increase mortality in patients with heart failure of ischaemic origin.
Isoprenaline (ββββ)
It acts on β1 and β2 receptors and increases heart rate and contractility. It’s main use is in significant heart blocks and bradyarrhythmias.
VASOPRESSOR: Vasopressin
Vasopressin (V1 V2)
Vasopressin acts on V1 and V2 receptors leading to vasoconstriction and increasing systemic vascular resistance. It also acts to increase renal water absorption. It may also have an effect on pulmonary vascular dilatation. It is a pure vasopressor and has no inotropic or chronotropic effect.
It has been used in cardiac arrest, but is primarily used in cases where there is shock secondary to vasodilatations such as in septic shock.
Some Important Comments in the Literature
Is one Pressor better than the other? Perhaps another question to ask is if one pressor, although efficacious in the short term lead to worst outcome? By this I mean, something that may work well right now, but lead to worst outcomes a week or two down the track when the patient is out of the emergency department.
The Cochrane Review first published findings in 2016 of Vasopressors in hypotensive shock and said”
“We found no evidence of substantial differences in total mortality between several vasopressors. Dopamine increases the risk of arrhythmia compared with norepinephrine and might increase mortality. Otherwise, evidence of any other differences between any of the six vasopressors examined is insufficient.”
Cochrane Database of Systematic reviews
Tarvasmaki et al, in an observational study in Critical Care (2016) 20:208 found that patients on Adrenaline had a worst survival and an increased 90 day mortality compared to other vasopressors. However the study didn’t prove causality and a prospective trial is needed.
In a comparison of Dopamine and Noradrenaline in the treatment of shock, De Baker et al (NEJM 2010;362(9):779) found that although not significant, there was a trend towards a higher death rate when Dopamine was used. There were certainly a significant number of adverse events such as arrhythmias, when Dopamine was used. In a sub-group analysis in this same study they found that in cariogenic shock, Noradrenaline was superior to dopamine in terms of reduction in mortality.
BACK TO THE CASES
CASE 1
This was the case of a 68 yo gentleman with SEPTIC SHOCK.
The medication options initially proposed are:
- Adrenaline
- Noradrenaline
- Dopamine
- Isoprenaline
- Dobutamine
- Milrinone
- Vassopressin
Lets remove some of these given that there is no issue with heart rate(isoprenaline goes) and at this point we assume no cardiac dysfunction, so we can remove inodilators, which leaves us with:
- Adrenaline
- Noradrenaline
- Vassopressin
The drug of choice to start with is NorAdrenaline. This is what we did. Following a period of improvement, the patient dropped his blood pressure again and became bradycardic. The ECG did not show any signs of ischaemia. Due to the continued bradycardia and hypotension, Adrenaline was added to help as both an inotrope and chronotrope, which solved the problem. With input from our ICU team we added Vasopressin as well and were able to significantly reduce the adrenaline.
CASE 2
This was the case of the 65 yo male in CARDIOGENIC SHOCK.
The optimal treatment for this patient would have been to start NorAdrenaline and then add Dobutamine, especially as there was no previous history of heart disease. Milrinone may be a substitute in patients with known poor ejection fraction ie., known significant heart failure.
The key is to start with Noradrenaline.
References
- De Baker D et al. Comparison of Dopamine and Norepinephrine in the treatment of shock. N Engl J Med 2010; 362:779-789
- Levy B, et al. Comparison of norepinephrine-dobutamine to epinephrine for hemodynamics, lactate metabolism, and organ function variables in cardiogenic shock. A prospective, randomized pilot study. Crit Care Med. 2011;39:450–5.
- Tarvasmaki T, et al. Current real-life use of vasopressors and inotropes in cardiogenic shock – adrenaline use is associated with excess organ injury and mortality. Crit Care. 2016;20:208
- Felker GM et al. Heart failure etiology and response to milrinone in decompensated heart failure: results from the OPTIME-CHF study. J Am Coll Cardiol. 2003;41:997–1003.
- Bistola V et al. Inotropes in Acute Heart Failure: From Guidelines to Practical Use: Therapeutic Options and Clinical Practice. Card Fail Rev. 2019 Nov; 5(3): 133–139
- Maggioni AP et al. EURObservational Research Programme: the Heart Failure Pilot Survey (ESC-HF Pilot) Eur J Heart Fail. 2010;12:1076–84








Keep this going please, great job!
My partner and I absolutely love your blog and find almost all of your post’s to be exactly
what I’m looking for. can you offer guest writers to write content
for yourself? I wouldn’t mind writing a post or elaborating on some of the subjects you write with regards to here.
Again, awesome web log!
my web-site A1 Keto
I genuinely enjoy looking at on this internet site, it has
got wonderful blog posts.
my website: Extreme Keto EFX Pills
It’s awesome designed for me to have a web page, whoch
iѕ useful in favor of my knowledge. thanks admin
I’d like to thank you for the efforts you have put in writing this site.
I’m hoping to check out the same high-grade content
by you later on as well. In fact, your creative writing abilities has encouraged me to get my own, personal blog now 😉
I simply could not depart your site prior to suggesting that I extremely enjoyed the standard information an individual supply for your guests? Is gonna be again continuously in order to check out new posts
Good day! Do you use Twitter? I’d like to follow you if that would be ok. I’m absolutely enjoying your blog and look forward to new updates.