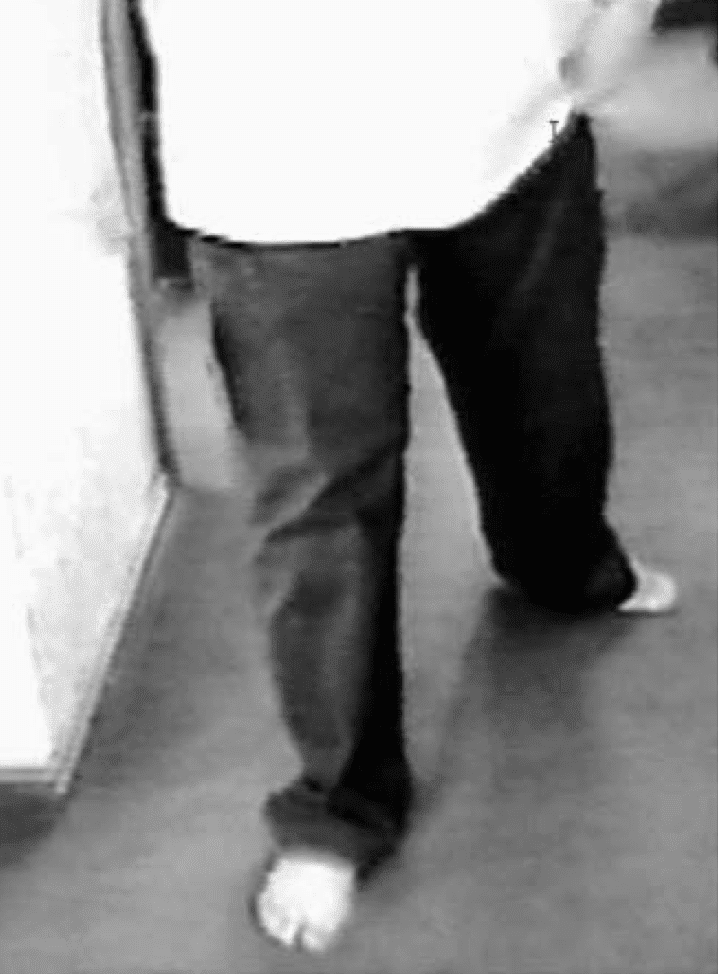
A 58 yo patient presents with weakness of the left leg. The patient states that the leg felt numb and weak last evening. He went to bed thinking it would improve, however this morning, it is the same, perhaps worst. He walks into the department dragging the whole leg behind him. He states that the leg feels like it doesn’t belong to him and he thinks he has had a stroke.
His past medical history includes hypertension, hypercholaesterolaemia, diet controlled diabetes and depression.
On examination: He is alert and well looking. On examination of the lower limb, tone is normal as are reflexes. There is sensory loss over the whole left leg that is demarcated at the groin and there is global weekness of the leg at 4/5.
Is this a stroke?
Could this be functional weakness?
Functional weakness can be a difficult diagnosis to make. It requires a good history and the clinical signs are crucial. The difficulty arises in that some patients with suspected functional weakness, are found to have an organic disease. Also, organic disease, is a risk factor for developing functional symptoms.
Patients can present acutely or with chronic and acutely worsening symptoms.
If there is more than monoplegia involved we need to keep in mind that this could be a stroke, or a stroke mimic. Mimics are usually not sudden in onset and do not restrict themselves to a vascular territory. Symptoms may also fluctuate in intensity.
The table below shows some characteristics that can differentiate stroke from mimics.

Differentiating stroke from stroke mimics
Characteristics of Functional Weakness
Functional weakness may be suspected in patients where the examination fluctuates and does not fit with stroke syndromes.
 Dragging of the whole leg, does not fit with a stroke as we would expected circumduction of the foot in a stroke, due to the hypertonia of the hip and the accompanying foot drop, that occurs.
Dragging of the whole leg, does not fit with a stroke as we would expected circumduction of the foot in a stroke, due to the hypertonia of the hip and the accompanying foot drop, that occurs.
In Functional Disease, patients may present with:
- Dragging the whole lower limb behind them
- Collapse of the knee, sometimes on soft touch. This can also apply to the upper limb which can collapse on soft touch.
- Fluctuations in the impairment during the examination
- Body swaying
- Positive Rhombergs, either falling away or towards the examiner.
What signs can help us diagnose functional disease?
We cannot depend totally on any one sign, to make the diagnosis and we should beware of making the diagnosis of functional disorder without discussion with Neurology, as this is such a complex area and signs that we think may be functional, may actually be organic. No sign can help us differentiate functional disorders from malingering.
Below we discuss the use of Pronator Drift and Hoover’s Sign.
Pronator Drift Sign
Refer to Pronator Drift Sign in a previous blog. Patients complaining of arm weakness are asked to hold their arms out in front of them with palms facing upwards. In real weakness of the arm, the arm drops slowly with associated pronation, because the pronators overpower the supinators. This is a very sensitive early sign for detecting arm weakness.
In patients with functional weakness or malingering, the arm simply lowers vertically without pronation.

J Neurol Neurosurg Psychiatry 2002;73:241–245
Hoover’s Sign
Hoover’s Sign is a motor test for functional weakness of the lower limbs. It relies on the cross extensor reflex. When one hip flexes, the contralateral hip extends, regardless of disease. Motor signs are more reliable than sensory signs in predicting functional weakness.
The sign can be performed in two ways:
Hip Extension: First test voluntary hip extension of the weak limb, by placing your hand under the patient’s heel. Then ask the patient to flex the normal hip. When the normal hip is flexed an involuntary extension of the affected limb occurs. If this involuntary extension is more powerful that the voluntary extension, it may indicate functional disease. There are some caveats.
Hip Flexion: This has not been validated. The patient is asked to flex the hip on the affected side, whilst the examiner places their hand under the heel of the normal leg. If the patient cannot flex the hip on the side of the affected side due to weakness but at the same time, no extension force is felt in the normal heel, it may indicate that the patient is not making an effort.
Caveat: False Positives and Negatives in Hoover’s Sign.
We need to be aware that pain can produce greater weakness and diseases such as multiple sclerosis can give false positive results. False negatives can also occur when the patient is not concentrating on flexing the normal hip.
References
- Buck B et al. Stroke mimics: incidence, aetiology, clinical features and treatment. Annals of Medicine. 2021;53(1):420-436.
- Stone J et al. Functional Weakness and sensory disturbance. J Neurol Neurosurgeon Psychiatry 2002;73:241-245
- Stone J et al. J Neurol Neurosurgeon Psychiatry 2005;76:(Suppl 1)







