Literature Review: Restriction of Intravenous Fluids in ICU Patients with Septic Shock. NEJM 386;26. June 30,2022 pp2459-2470.
In patients with septic shock, higher volumes of intravenous fluids have been associated with worst outcomes. These included kidney injury, respiratory failure and an increased risk of death. Most of these conclusions came from randomised trials and observational studies. The quality of this evidence has not been high and a recent review of meta-analysis has resulted in a rethink.(1)
The surviving sepsis campaign initially recommended a 30ml/kg fluid bolus. There is no current recommendation for ongoing fluids following initial resuscitation. Enter the CLASSIC Trial: The Conservative versus Liberal Approach to Fluid Therapy of Septic Shock in Intensive Care.
Study Design
Open Label, Randomised Trial conducted internationally in 31 ICU’s in Europe.
Primary Outcome: Death from any cause within 90 days of randomisation.
n= 1531
The patients were chosen if >18yo and in ICU and had septic shock.
Septic Shock was defined as:
- Suspected or Confirmed Infection
- Plasma Lactate of >2mmol/L
- Ongoing infusion of vasopressor or inotrope
- > 1Litre of intravenous fluid in the 24 hours before screening
Randomisation: This was into two groups:
- Restrictive Fluid Group
- Standard Fluid Group
Restrictive Fluid Group
In this group intravenous fluids could only be given under 4 conditions
- If the patient had severe hypo perfusion as defined below, they could receive 250-500mL bolus of isotonic crystalloid
- Plasma lactate>4mmol/L
- MAP of < 50mmHg despite pressor or inotropes
- Mottling beyond the edge of the kneecap(mottling score > 2)
- Urine output < 0.1ml/kg/hr, during the first 2 hours after randomisation
- To replace documented fluid losses
- To correct dehydration or electrolyte deficiency
- To ensure daily fluid intake of 1 liter
Standard Fluid Group
There was no limit to the amount of fluid that this group could receive. Intravenous fluids could be administered in the following circumstances:
- For as long as the patient’s haemodynamic factors improved
- To replace expected or observed losses or to correct dehydration or electrolyte abnormalities
- Maintenance fluid, if the ICU involved had a protocol for it.
RESULTS
The trial period lasted for 90 days, although both groups remained in ICU for a median period of 5 days following randomisation.
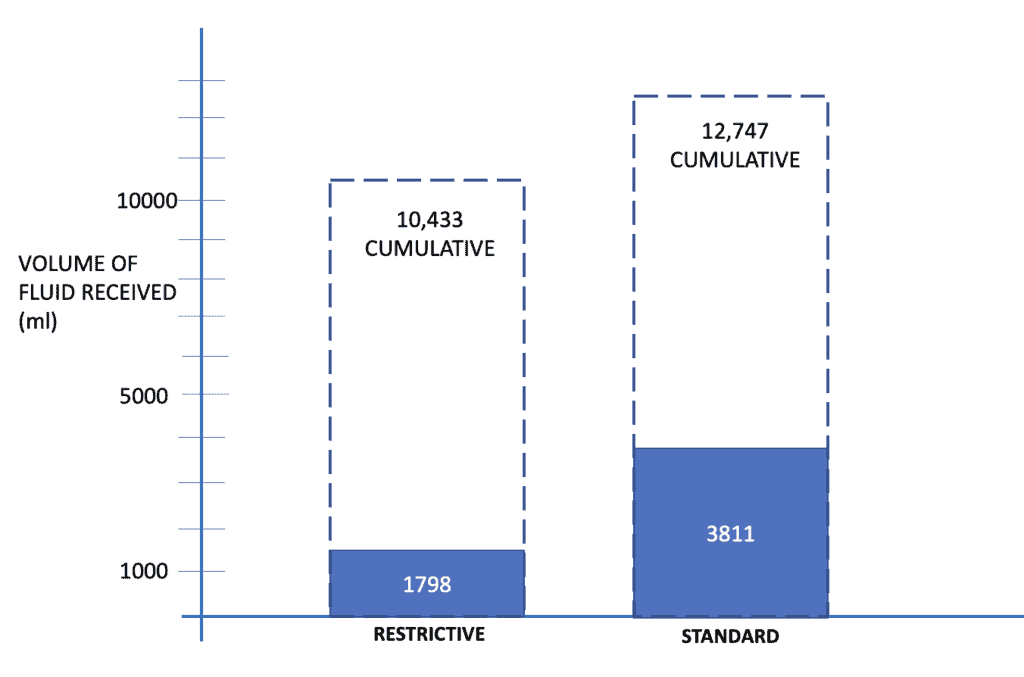
The amount of fluid received in the two groups was:
- 1798ml in the restrictive group, with a cumulative total of 10433 ml
- 3811ml in the standard group with a cumulative total of 12747 ml
The amount of fluid given for ongoing loses was similar in the two groups. The main difference seen was the amount given in fluid boluses.
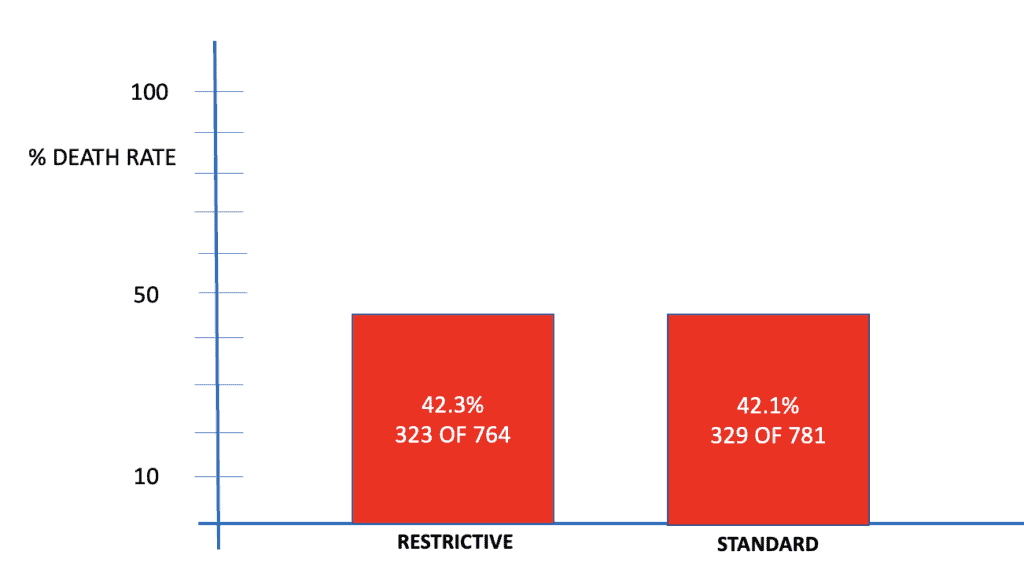
The death rates at 90 days, in the two groups were very similar as seen below.
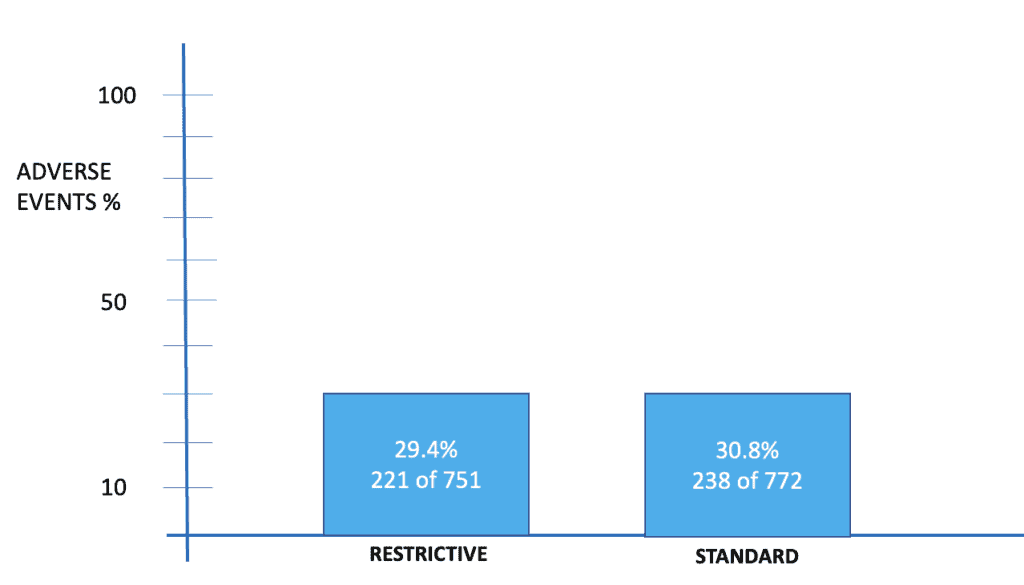
The % of adverse events in the two groups was also similar.
Conclusion
There were no significant differences in 90 day mortality or in serious adverse events between the two groups.
This study result is similar to a meta analysis in Chest(2), asking the same question.
References
- Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med 2021;47:1181-247.
- Meyhoff TS, Møller MH, Hjortrup PB, Cronhjort M, Perner A, Wetterslev J. Low- er vs higher fluid volumes during initial management of sepsis: a systematic re- view with meta-analysis and trial sequen- tial analysis. Chest 2020;157:1478-96.







